-
Email [email protected]
-
Address 848 N. Rainbow Blvd. #5486 Las Vegas, NV 89107, USA
1Georgia Heart Institute, Gainesville, Georgia, USA.
2Department of Internal Medicine, Northeast Georgia Medical Center, Gainesville, Georgia, USA.
*Corresponding author: Priyadarshini Dixit & Shivani Mehta
Georgia Heart Institute, Gainesville, Georgia, USA.
Email ID: [email protected] & [email protected]
Received: Nov 05, 2024
Accepted: Dec 02, 2024
Published Online: Dec 09, 2024
Journal: Annals of Cardiology
Copyright: © Dixit P & Mehta S et al. (2024). This Article is distributed under the terms of Creative Commons Attribution 4.0 International License
Citation: Dixit P, Mehta S, Patel S, Kilaru V, Adams A, et al. Congenital absence of right coronary artery: A rare congenital malformation. Ann Cardiol. 2024; 1(1): 1001.
Congenital absence of Right Coronary Artery (RCA) is a rare congenital malformation of the cardiovascular system with serious implications to health including acute myocardial infarction and death. Early diagnosis and prompt intervention in these selected patients can prevent cardiovascular complications. We are presenting a case of a 60-year-old male who presented to our outpatient clinic with shortness of breath on exertion. Upon cardiac evaluation, he was found to have congenital absence of Right Coronary Artery with 80% obstructive stenosis of the Left Circumflex coronary artery. He subsequently underwent successful percutaneous coronary artery intervention as an outpatient procedure and was discharged home in stable condition.
Keywords: Right coronary artery; Congenital malformation; Single coronary artery.
Congenital absence of Right Coronary Artery (RCA) is a rare congenital malformation with very few documented cases. Although it is a benign anomaly, it can be associated with serious cardiovascular complications which includes acute myocardial infarction, stroke, and even death [1]. It is thought to be due to an abnormal embryonic developmental defect or congenital occlusion of the coronary artery [2]. When these patients present with cardiac symptoms, prompt recognition with appropriate diagnostic evaluation is needed to prevent cardiovascular complications. Coronary Computed Tomography Angiography (CCTA) is an excellent modality with high accuracy in diagnosing anomalous coronary artery in addition to a single coronary artery in selected patients.
We present to you a case of a 60-year-old male with history of hypertension and hyperlipidemia who presented to our outpatient clinic with shortness of breath on exertion for several weeks. He underwent cardiac evaluation with CCTA and was diagnosed with congenital absence of RCA and an obstructive lesion in the Left Circumflex artery (LCx). Due to early detection and diagnosis, he underwent successful Percutaneous Coronary Intervention (PCI) and was discharged in a medically stable condition.
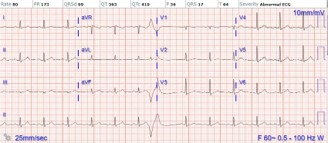
60-year-old male with history of hypertension and hyperlipidemia was referred to our outpatient clinic by his primary care provider for abnormal Electrocardiogram (ECG) with Premature Ventricular Complexes (PVCs) and shortness of breath on exertion. Shortness of breath occurred with minimal exertion and was not associated with chest pain or discomfort. He did admit to a history of tobacco use and was on an inhaled Short Acting Beta Agonist (SABA) rescue inhaler. The patient’s symptoms persisted, and he became worse despite treatment with a SABA rescue inhaler. He denied any family history of premature coronary disease and was compliant with other cardiac medications. During the visit, Blood Pressure (BP) was 130/80 mmHg, Heart Rate (HR) was 80 bpm, and BMI was 28.59 kg/m2. ECG demonstrated sinus rhythm with abnormal R wave progression with early transition and the presence of PVCs (Figure 1). Given his risk factors and clinical symptoms, Transthoracic Echocardiography (TTE) and a nuclear treadmill stress were ordered as outpatient tests.
TTE showed normal Left Ventricular Ejection Fraction (LVEF) of 55-60% with no significant valvular pathology and normal LV filling pressures. A nuclear treadmill was performed to assess for myocardial perfusion ischemia defects. The patient exercised on Bruce protocol for a total of 8 minutes, 48 seconds and achieved 10.4 METS with 93% MPHR. Stress ECG was negative for ischemia, however nuclear perfusion showed a mixed perfusion defect in the basal to apical inferior segments (possibly suggestive of ischemia in the RCA territory) versus a diaphragmatic attenuation artifact. Given that ischemia could not be completely ruled out with moderate probability of Coronary Artery Disease (CAD), further coronary ischemia investigation was performed with a CCTA to define the coronary anatomy and evaluate for evidence of obstructive CAD.
CCTA revealed the absence of RCA, a large dominant LCx with first Obtuse Marginal (OM 1), OM 2, OM 3 and a small posterior descending artery (PDA) which wrapped around the right atrioventricular (AV) groove and terminated anteriorly ending near the aorta as right ventricular branch. Proximal LCx demonstrated 50-70% stenosis and the proximal LAD with >70% calcific stenosis. Fractional flow reserve (FFR) of the LCx was 0.52 and LAD 0.80. Total calcium score 2635, LM 204, LAD 1316, LCx1115.
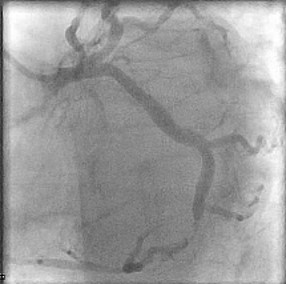
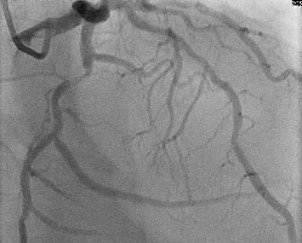
Patient was informed of these high-risk findings on CCTA with evidence of obstructive CAD and the decision was made to proceed with the gold standard left heart catheterization with coronary angiography to ensure accuracy of the obstructive lesion and intervention if the lesion was found to be obstructive. Cardiac catheterization revealed an obstructive lesion of the mid LCx with 80% calcified stenosis and he underwent successful Intravascular Ultrasound (IVUS) guided PCI of the LCx with pre and post balloon angioplasty utilizing a 3.5x22 and 3.0x15 mm overlapping Onyx frontier Drug-Eluting Stent (DES). LAD lesion angiographically appeared to be non-obstructive and medical management was elected (Figures 2-4).
Patient was monitored overnight in the cardiac critical care unit (CCU). He remained hemodynamically stable. The next day, he was discharged home in medically stable condition on 81 mg ASA daily, prasugrel 10 mg daily, atorvastatin 40 mg daily, and metoprolol succinate XL 25 mg daily.
During his follow up visit after one week, the patient stated that his shortness of breath on exertion had resolved and he reported compliance with his Dual Antiplatelet Therapy (DAPT) with no bleeding issues.

A Single Coronary Artery (SCA) is described as an isolated coronary artery that arises from the aortic trunk by a single coronary ostium [3]. It is a rare congenital anomaly with a prevalence of 0.014%-0.066% of the general population [1]. It is thought to be due to abnormal embryonic development related to a fetal developmental defect or congenital coronary occlusion [2]. The angiographic classification of SCA was first proposed by Lipton et al in 1979 and is now widely used in clinical practice [4]. In brief, it is classified by site of origin (right or left coronary sinus), anatomical distribution of branches (groups I, II, and III), and the course of the transverse trunk (A-anterior, B-between, and P-posterior) in relation to the aorta and pulmonary artery. Congenital absence of the right coronary artery (RCA} is a subtype of SCA and was first described by White and Edwards in 1948 [5].
Individuals with congenital absence of the RCA can present with a wide variety of clinical manifestations, ranging from asymptomatic to life threatening symptoms including myocardial infarction, syncope, and arrythmias [6]. Younger patients may not show initial signs and symptoms of this anomaly due to lack of confounding cardiovascular risk factors such as atherosclerosis, hypertension, or diabetes. However, with age and progressive atherosclerosis contributing to coronary artery disease, these patients will often exhibit symptoms of angina pectoris, myocardial infarction, syncope, cardiac arrhythmias, congestive heart failure, and sudden cardiac death [7]. This pathogenesis could be attributed to excessive dilatation of the single coronary artery due to increased tension on the vessel in the setting of increased metabolic demands in supplying perfusion to the heart. This increased tension predisposes to endothelial injury, triggering the atherosclerotic process and chronic local inflammation [2]. Therefore, it is imperative that accurate and timely diagnosis is made. ECG manifestations of patients with absence of the RCA vary, with one study showing that 60% of patients with RCA absence have ST-T segment changes on ECG and half of the patients have obvious lesions in the left coronary artery branches [8]. Other manifestations include atrioventricular blocks, sinus bradycardia, atrial fibrillation, and various supraventricular arrhythmias. Because the sinoatrial (SA) and Atrioventricular (AV) node are typically supplied by the RCA, patients with this unique anatomy rely on the left coronary artery or left circumflex artery for long-term perfusion. Lack of adequate blood supply ultimately leads to ischemia of the SA and AV node, eventually resulting in fibrosis and subsequent dysfunction [2,8].
While congenital coronary anomalies are considered rare, they can exhibit familial clustering, suggesting a genetic component to their etiology [9]. Family history assessment and genetic testing may be warranted in cases of congenital coronary anomalies to identify potential hereditary predispositions and inform risk stratification for affected individuals and their relatives. Additionally, screening of first-degree relatives for coronary anomalies and associated cardiovascular risk factors may aid in early detection and preventive interventions, thereby mitigating the risk of adverse cardiovascular events in susceptible individuals. Through comprehensive family-based approaches, including genetic counseling and lifestyle modifications, efforts can be made to reduce the burden of congenital coronary anomalies and optimize cardiovascular health across generations.
A diagnostic coronary angiography is considered the gold standard for diagnosing a SCA. However, this modality has limitations such as long operation time, increased contrast exposure, and misdiagnosis. Technological advances have allowed us to better detect these congenital anomalies through coronary artery Computed Tomography Angiography (CCTA) due to its wide availability, noninvasive nature, and high accuracy [9]. CCTA provides a three-dimensional picture of the coronary vasculature and provides anatomical relationship to other cardiac structures. Many studies have concluded that CCTA should be the first-choice imaging modality for patients in whom coronary artery anomalies are suspected [10-12]. There is currently no standardized treatment for congenital absence of the RCA. Conservative management with anti-platelets or lipid-lowering agents may be used in asymptomatic patients, whereas patients presenting with acute myocardial infarction would benefit from percutaneous coronary intervention or coronary artery bypass surgery [2]. In our case, the patient presented with progressive angina and was diagnosed with congenital absence of the RCA via CCTA. The patient subsequently had stent implantation in the distal LCx artery with improvement in anginal symptoms.
This case report outlines the unique presentation of a patient diagnosed with congenital absence of the right coronary artery, a rare anomaly with significant implications for cardiovascular health. Successful management of this patient through PCI underscores the importance of early detection, thorough multimodal evaluation, and prompt intervention. The utilization of CCTA highlights the crucial role of advanced imaging modalities in identifying and guiding therapeutic approach. As our understanding of congenital coronary anomalies continues to advance, we call for further research into these topics to identify primary prevention strategies, optimal management, and long-term outcomes.
