-
Email [email protected]
-
Address 848 N. Rainbow Blvd. #5486 Las Vegas, NV 89107, USA
1Division of Community Medicine, Mercer University School of Medicine, Columbus, GA 31901, USA.
2Charter Radiology, Columbia, MD 21044, USA.
3Mangat & Kaur INC Germantown, MD 20876, USA.
*Corresponding author: Abraham M Enyeji
Division of Community Medicine, Mercer University School of Medicine,
Columbus, GA, 31901, USA.
Email ID: [email protected]
Received: Oct 28, 2024
Accepted: Dec 23, 2024
Published Online: Dec 30, 2024
Journal: Annals of Cardiology
Copyright: Enyeji AM et al. © All rights are reserved
Citation: Enyeji AM, Kathuria S, Spencer Hammett B, Nimi T, Mangat HS. Vaccine injury following moderna COVID-19 vaccine: A case report. Ann Cardiol. 2025; 1(1): 1003.
Following the proliferation of the SARSCoV-2 virus worldwide, there has been urgent demand for the rapid development of vaccines. Consequently, years following the identification of the virus, multiple vaccine candidates were formulated and authorized for distribution. In response to the rising number of individuals experiencing uncommon adverse effects postvaccination, not explicitly outlined in product specifications, the Centers for Disease Control and Prevention introduced V-Safe, a real-time Vaccine Adverse Event Reporting System (VAERS), to meticulously monitor potential adverse effects arising from the vaccines. Given this context, we present a case of coronary artery occlusion and internuclear ophthalmoplegia following the administration of the Moderna COVID-19 mRNA vaccine. This case underscores the importance of closely monitoring patients reporting a variety of symptoms, such as chest discomfort and unclear vision or loss of vision post-vaccination, particularly if they do not respond to standard treatment.
Keywords: SARS-CoV-2 virus; Modern a COVID-19 vaccine; CT angiogram.
The global pandemic caused by Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) has led to the widespread occurrence of Coronavirus Disease 2019 (COVID-19), affecting multiple body systems. In response, the United States Food and Drug Administration authorized the emergency use of the Moderna COVID-19 vaccine (mRNA-1273 SARS-CoV-2) at the end of 2020 [1]. While venous thromboembolism is rarely linked to mRNA vaccines, there have been reports of uncommon thrombotic events, including Vaccine-Induced Thrombotic Thrombocytopenia (VITT) and arterial thrombosis such as Central Retinal Artery Occlusion (CRAO), following the Moderna mRNA-1273 vaccination [2]. These events have been noted due to a temporal association between vaccination and the occurrence of CRAO [3]. This report discusses a case involving diplopia, atypical carotid artery occlusions, and coronary artery occlusion that appears to be linked to the Moderna COVID-19 vaccine.
A 65-year-old Caucasian male, previously in good health, presented with vertigo, lightheadedness, and diplopia that began the previous night at 11:23 PM. He reported that his vision initially became blurry and then progressed to double vision. He also experienced mild dysphagia, which began that night but allowed for the tolerance of liquids. Upon waking the next day, his symptoms had worsened, prompting his visit to the emergency room, where left internuclear ophthalmoplegia was identified via imaging. Additional complaints included loss of balance with unsteadiness while walking and stuttering, which were confirmed by his wife and son to be unusual for him. He denied chest pain, palpitations, chills, shortness of breath, aphasia, or syncope. Although he admitted to regular alcohol consumption, he denied any history of alcohol withdrawal symptoms and illicit drug use. His medical history included treatment for COVID-19 on May 23, 2023, with Kaletra, Hydroxychloroquine (HCQ), Pulmicort, famotidine, clarithromycin, and Benadryl. He received the Moderna COVID-19 vaccination on May 5 and June 2, 2023.
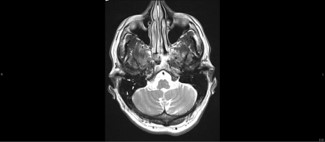
In the emergency room, his vitals indicated hypertension, with otherwise stable parameters. His EKG showed normal sinus rhythm at 73 bpm with an incomplete left bundle branch block. Carotid Doppler and CT angiography of the neck revealed 69% stenosis of the left carotid artery as shown in Figure 1 above, and less than 20% stenosis of the right carotid artery (Figure 2). He was started on Plavix and maintained on oral doses.

During his initial office visit, he presented with diplopia when looking outward horizontally and downward to the right. He also experienced difficulties typing and spelling, despite being a childhood spelling champion. His D-dimer level was elevated at 0.88 (normal range 0-0.49), and CRP was within normal limits at 1 (<1.0 mg/dL). His COVID-19 spike protein antibody level was initially >3385 Arbitrary Units per milliliter (AU/ml) (normal range <0.8 AU/ml).
A CT angiography of the heart revealed extensive moderate stenosis in the proximal left anterior descending coronary artery and severe stenosis in the mid left anterior descending coronary artery. Notably, the occlusion was in the mid artery with a clear view to the capillary walls. He underwent catheterization with stent implantation in the culprit lesion and was provided with an appropriate secondary preventive medication regimen.
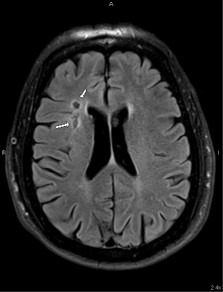
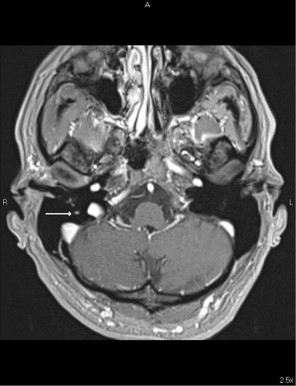
An accompanying 3T MRI showed contrast enhancement in the right facial nerve with mastoid effusion, a condition associated with COVID-19 [4,5]. Effusions on the mastoid of COVID-19 patients, thickening of the facial nerve, and subarachnoid space closure on the facial nerve were noted (Figures 2, 3 & 4). He was started on ivermectin 13 mg for 10 days and subsequently every month. His diplopia resolved within a month, and his feet felt warmer.

Cardiovascular complications associated with COVID-19 have gained attention due to their prevalence and severity, including conditions such as myopericarditis, Takotsubo cardiomyopathy, myocardial infarction, and venous thromboembolism [6]. Among these complications, common carotid artery occlusion (CCAO) is less frequently documented, with many cases remaining asymptomatic. Existing studies report CCAO incidence rates of 0.24% to 0.54%, with the condition occurring in 1%-5% of stroke cases, predominantly affecting the right side [7]. Our case presented an atypical manifestation, where the left CCAO was notably more severe than the right, prompting further investigation into a potential COVID-19 connection.
This unusual severity of carotid occlusion, coupled with the patient’s history of cardiovascular complications commonly associated with COVID-19, suggested a possible link. The hypercoagulable state seen in COVID-19 patients may result from systemic inflammation and endothelial injury induced by the virus, alongside increased pro-coagulant factors [8,9]. Autopsy studies have highlighted the high prevalence of thromboembolic events, reinforcing the idea that COVID-19 significantly affects coagulation pathways [10]. In our patient, the extensive occlusions observed in the left anterior descending artery, and the internuclear ophthalmoplegia were particularly concerning, especially given their history of SARS-CoV-2 vaccination, which may exacerbate thrombus formation. Previous authors have described the clinical manifestations and short-term prognosis of ocular motility disorders such as internuclear ophthalmoplegia [11,12].
The interaction between heparin and the SARS-CoV-2 spike protein presents an additional layer of complexity. Notably, the COVID-19 spike protein exhibits a high affinity for heparin, which can enhance thrombotic conditions, particularly in narrowed arterial spaces, such as the severely stenosed left carotid artery in our patient. This potential for increased thrombogenic activity underscores the critical need for careful monitoring of anticoagulant therapy in the context of COVID-19. Conversely, ivermectin mitigates these risks by preventing the spike protein from interacting with host cell membranes, thereby reducing viral entry and replication [13].
Additionally, MRI findings in our patient indicated cranial nerve lesions associated with COVID-19. Previous studies have documented cranial nerve involvement, including anosmia linked to the olfactory bulb and facial nerve paralysis [14-16]. This raised concerns about potential vaccine injury, particularly given the evidence linking vaccine-induced inflammation and thrombosis [17].
The combination of confirmed thrombus formation in the coronary arteries via CT angiogram and elevated serum spike protein antibody levels supported the hypothesis of vaccine-induced thrombotic events, rather than simple plaque formation. Furthermore, the administration of ivermectin for over four months led to notable improvements in the patient’s symptoms, with a documented reduction in COVID-19 spike protein levels from 3385 arbitrary units per milliliter (AU/ml) at presentation to 2699 AU/ml. This decline further illustrates the potential therapeutic benefits of ivermectin. Overall, these findings suggest that the occlusion was primarily caused by elevated viral spike protein rather than the conventional pathways associated with atherosclerotic disease.
In conclusion, this case highlights the significant risk of thrombotic events following vaccination with the Moderna COVID-19 vaccine, particularly in patients with preexisting conditions. The interplay between heparin and the spike protein underscores the need for careful monitoring and individualized treatment strategies in such cases. The observed cranial nerve lesions and visual defects emphasize the importance of being vigilant about neurological complications related to COVID-19 and its vaccination. Further research is crucial to elucidate the mechanisms behind vaccine-induced thrombosis and to develop guidelines that optimize patient outcomes while ensuring the safe administration of vaccines to vulnerable populations.
Ethical considerations: Ethical considerations and consent are not applicable, as there were no relevant factors requiring them.
Consent to participate: The authors confirm that informed consent was obtained from all participants involved in this study.
Consent for publication: Informed consent was obtained from all subjects involved in the study.
Funding: This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflicting interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability: For this case report, patient data, including laboratory findings and imaging studies, can be obtained from the authors upon request.
