-
Email [email protected]
-
Address 848 N. Rainbow Blvd. #5486 Las Vegas, NV 89107, USA
1Western Sydney University, Australia.
*Corresponding author: Alan Silburn
Western Sydney University, Campbelltown, 2560, NSW, 2 Lawn Avenue,
Robertson 2577, Australia.
Email ID: [email protected]
Tel: 0449-107-944
Received: Jan 04, 2025
Accepted: Feb 10, 2025
Published Online: Feb 17, 2025
Journal: Annals of Cardiology
Copyright: Silburn A et al. © All rights are reserved
Citation: Silburn A. Scoping review: Deciphering the best defense against cardiovascular events in hypertensive adults. Ann Cardiol. 2025; 2(1): 1005
Hypertension is a critical risk factor for cardiovascular events, affecting one in three adults globally. This scoping systematic review compares the efficacy of Angiotensin-Converting Enzyme Inhibitors (ACEi) and diuretic-class medications in reducing cardiovascular event risk in hypertensive adults. The review synthesises findings from two randomised controlled trials and a meta-analysis, revealing conflicting results. While diuretics demonstrate superiority in preventing major cardiovascular diseases, ACE inhibitors are favoured for minimising neurological deficits post-stroke and reducing overall cardiovascular risk. These findings underscore the need for personalised antihypertensive therapy and highlight the complexity of establishing a singular optimal treatment standard.
Keywords: Hypertension; Cardiovascular events; ACE inhibitors; Diuretics; Antihypertensive therapy; Stroke prevention.
The World Health Organisation [2] defines hypertension as a condition in which the blood vessels have persistently raised pressure. Considered both a disease and a major risk factor for disease, hypertension remains one of the major contributors to premature death worldwide [2]. Population studies demonstrate that the rate of a cardiovascular event such as stroke or myocardial infarction exponentially rises with increased systolic blood pressure [3].
Although its burden is experienced globally, first-line management of hypertension remains a topic of debate amongst healthcare providers [4]. Historically, the use of Angiotensin-Converting Enzyme inhibitors (ACEi) as the primary management for hypertensive patients has had significant inquiry relating to the intervention’s association with a favourable outcome when compared to diuretic agents [4,5]. Most commonly, outcomes were characterised in two forms: the associated risk of cardiovascular disease morbidity and mortality [2,5]; or the stability of blood pressure within standardised values commonly adjusted for age, gender, and ethnicity [6].
The current standard of care for managing hypertension involves the use of combination therapy for most patients. However, exceptions exist where monotherapy of any of the four classes of drugs – diuretics, ACE-I, ARB or CCB, can be used as a first-line therapy, particularly in cases of elevated blood pressure within the range of 120/70 to 139/89 mmHg, moderate to severe frailty, symptomatic orthostatic hypotension, or in individuals aged 85 years or older. This article focuses on the role and considerations of monotherapy in hypertension management, exploring its relevance in these specific scenarios and assessing its effectiveness in achieving optimal patient outcomes [7].
Research question
Hypertension, a major risk factor for cardiovascular events such as cerebral or myocardial infarction, currently affects one in three people aged 18 years and over [1]. Of the many ways to manage hypertension, the administration of angiotensin-converting enzyme inhibitors or diuretic-class medications is common yet the determination which remains the golden standard is contested as both have different modalities of achieving blood pressure control. From this, the following PICO question was derived:
PICO Question: In adult patients with hypertension, what is the effect of angiotensin-converting enzyme inhibitors compared to diuretic class medications on cardiovascular event risk?
Search strategy
For this review, the Ovid Medline Complete and PubMed databases will be utilised as both have proven worth producing credible literature covering a wide range of scientific, medical, and healthcare disciplines [8] thus adequate for the proposed research question.
Inclusion and exclusion criteria
For the proposed, a quantitative methodology will be applied to determine cardiovascular event risk over the perception or experience of disease burden. Articles were considered for inclusion provided they were of quantitative design, remained after the screening, and no exclusion criteria were identified.
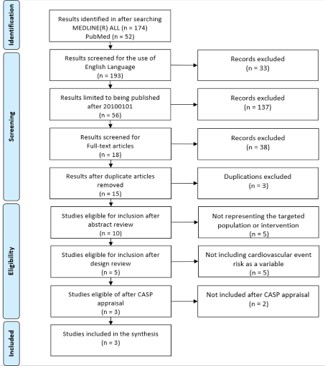
After the preliminary search, screening was possible by using the search engine limiters for literature published in the English language and published since 1st January 2010 to ensure currency. Although 10 years is preferred regarding timeframe, this limiter considers the approximate two-year reduction in research capability impacted by the Coronavirus Pandemic [10]. Additional screening was conducted limiting to full-text academic journals to ensure quality. Given the reduced pool, article duplicates were identified and removed. The first-pass exclusion was conducted by assessing the article’s abstract for comparability eliminating any non-comparable intervention or population characteristic. Second-pass exclusion occurred by assessing the study design ensuring that cardiovascular event risk was identifiable as a numerical variable. Of the articles remaining, all were assessed for quality and potential bias using the Critical Appraisal Skills Programme [11] appraisal methodology. Of these, the highest quality quantitative articles were included in the review. This process is further displayed in Figure 1: PRISMA diagram [12].
To generate a valid script, the terms need to be contemplated to ensure the results are relevant whilst not being over-limited. To achieve this, a PICOT framework [9] was utilized to refine the key components being tested with the results displayed in Table 1.
| Keywords/search terms/phrases | Alternative words/terms considered | |
|---|---|---|
| P | Adults with hypertension | Adult/ aged 18 years/ patient; hypertension/ high blood pressure |
| I | Angiotensin-converting enzyme inhibitors | ACE inhibitors/ Perindopril/ Quinapril/ Antihypertensive |
| C | Diuretic class medications | Diuretic/ thiazide/ loop/ potassium-sparing/ osmotic/ carbonic anhydrase inhibitors |
| O | Cardiovascular event | Cardiovascular event/ stroke/ cerebrovascular accident/ heart attack/ myocardial infarction |
| T | Between 2010-2023 | 20100101 – 20230512; since 2010 |
((adult* 20100101 – 20230512; since 2010 OR patient*) AND (Angiotensin-converting enzyme inhibitors OR ACE inhibitors) AND Diuretic*).af. AND hypertension.sh. AND (cardiovascular disease OR stroke OR cerebrovascular accident OR heart attack OR myocardial infarction).sh.
Once selected, search terms were either combined with truncation methods and Boolean operators or controlled with Medical Subject Headings in a strategic means to produce relevant results for possible inclusion. This resulted in the following search action:
The quantitative articles included display similar attributes worthy of inclusion whilst also different in research design, sample size, population demographics, and intervention modality. A summary of the included articles is outlined in Table 2.
| ID; Author; Year Published; Country | Study design | Population/sample size | Population characteristics | Intervention variable | Comparison variable |
|---|---|---|---|---|---|
| 1. Einhorn et al, 2010; USA [13] | RCT double blinded | Total=42 418 Diuretic=15 255 ACEi=9 054 CCB=9 048 |
North American Mixed gender Aged 55 years or older |
Chlorthalidone, 12.5 to 25 mg/d | Lisinopril, 10 to 40 mg/d |
| 2. Maïer et al, 2022; USA [15] | Post hoc analysis of RCT | Total=203 ACEi=126 Diuretic=79 CCB=68 BB=106 |
French Mixed gender Aged 18 years or older |
ACEi, Potential bias: nondisclosed dose/mg | Diuretic Potential bias: nondisclosed dose/mg |
| 3. Xie et al; 2018; China [17] | Meta-Analysis of 27 RCTs | Total=143 095 ACEi=18 282 Diuretic=3 073 CCB=5 313 BB=1 104 ARB=13 100 Placebo=102 223 |
International Mixed gender Aged 18 years or older |
ACEi vs. Placebo Potential bias: nondisclosed dose/mg | Diuretic vs. Placebo Potential bias: nondisclosed dose/mg |
Note: Values are expressed as numbers (n=) unless otherwise indicated. ACEi indicates angiotensin-converting enzyme inhibiter; CCB: Calcium Channel Blocker; BB: β-blockers; ARB: Angiotensin Receptor Blocker.
The synthesis encompasses two randomized controlled trials and a systematic review/meta-analysis of high-level evidential strength that evaluates different antihypertensive therapies and their impact on cardiovascular events, neurological deficit, and overall risk reduction.
Article 1 [13] reports on the Antihypertensive and Lipid Lowering Treatment to Prevent Heart Attack Trial -ALLHAT [14], a double-blind RCT comprising over 42,000 participants aged 55 years or older from North American centres. Participants were randomly assigned to one of three arms: Diuretic; Calcium channel blocker; or ACEi in a ratio of 1.7:1:1 for statistical power towards the diuretic arm with a planned follow-up ranging from 4 to 8 years. The outcome was measured as the incidence of combined fatal and nonfatal cardiovascular events. Following analysis, the authors concluded in favour of diuretics being superior in preventing one or more major forms of cardiovascular disease and is the preferred first-line therapy for patients with hypertension.
In contrast, Article 2 [15] presents a post hoc analysis of the BPTARGET trial [16], a multicentre blind-assessed trial conducted at over 200 French facilities. The study evaluates the effect of different antihypertensive therapies on neurological deficit severity after stroke in hypertensive patients. Participants were randomly assigned, in a 1:1 ratio, to have ‘tight’ systolic blood pressure control (100-129 mmHg) or ‘conservative’ control (130185 mmHg) during the following 24-36 hours. Participants were followed up at 2and 3 months for neurological deficit scoring and ischemic core measurement by neuroimaging. The post hoc findings concluded that the neurological deficit score differed in severity according to the antihypertensive used. Contrary to Article 1 [13], the authors concluded in favour of ACEi as the preferred first-line method for reducing neurological deficit severity after stroke in hypertensive patients when compared to diuretics.
Article 3 [17] presents a systematic review and meta-analysis of 27 RCTs with participants from different countries. The study assesses the effectiveness of different antihypertensive therapies in reducing cardiovascular event risk. The study used a robust and replicable search strategy within multiple databases. Inclusion was stringent and targeted mono vs placebo, and mono vs mono antihypertension therapies. Unfortunately, like Article 2 [15], the pharmacology and dosing regimen were not identifiable. Although the ACEi arm was largely represented in comparison to diuretics at a ratio of 5.95:1, the generated mono vs placebo risk ratio was comparable. From this, the authors also concluded in favour of diuretics, RR=0.77 (95% CL 0.66-0.90), over ACEi, RR=0.85 (95% CL 0.78-0.92), when compared against a placebo arm as the primary method of hypertension management to reduce cardiovascular event risk.
Taken together, these findings have important clinical implications and highlight the need for appropriate antihypertensive therapy to optimise risk reduction and improve patient outcomes.
A major risk factor for diseases, hypertension remains one of the global targets for non-communicable diseases as it is a major contributor to premature death worldwide [2]. Although its burden is experienced globally, first-line management of hypertension remains a topic of controversy and debate amongst healthcare providers [4].
Overall, the studies presented suggest that antihypertensive therapies play a vital role in reducing cardiovascular event risk and neurological deficit severity after stroke in hypertensive patients. While some suggest diuretics are superior in preventing major forms of cardiovascular disease, others proclaim ACEi are preferred for reducing neurological deficit severity after stroke and are the primary method of hypertension management to reduce cardiovascular event risk. From this, the determination of a single golden standard treatment for hypertension remains elusive. Thus, treatment must remain patient-based with tailored antihypertensive treatment pertinent to the individual risk.
Limitations affecting the outcome may have arisen due to a narrowed field restricted by design. Additionally, the medication/dose regime, though similar, was not defined fostering potential measurement bias. Further enquiry into this subject should consider a broader inclusion protocol with defined medication criteria.
Areas for future research
Future research in hypertension management could focus on comparing different antihypertensive medications mono vs mono in terms of their effectiveness and impact on cardiovascular event risk under blinded RCT conditions. Additionally, long-term follow-up studies could provide insights into how antihypertensive therapies are used in routine clinical practice and identify barriers to optimal management. Overall, future research should aim to optimise hypertension management and improve patient outcomes by further comparing ACEi and diuretics to cement a golden standard of treatment. Furthermore, different popular antihypertensives need to be compared with emerging therapies to encourage progression in this field.
Ethics approval and consent to participate: This study did not require ethical approval as it involved a retrospective analysis of publicly available and anonymized information, with no direct involvement of human subjects.
Consent for publication: The author consents for the publication of this article.
Availability of data and materials: Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
Competing interests: The author declares that they have no known competing interests or personal relationships that could have appeared to influence the work reported in this paper.
Funding: The author declares that they did not receive funding for this article.
Author’s contributions: The author solely contributed to the conception, design, analysis, and drafting of the manuscript.
