-
Email [email protected]
-
Address 848 N. Rainbow Blvd. #5486 Las Vegas, NV 89107, USA
1Department of Emergency Medicine, New York-Presbyterian/Columbia University Irving Medical Center, Columbia Vagelos College of Physicians and Surgeons, New York, USA.
2Emergency Medicine, New York-Presbyterian/Weill Cornell Medicine, New York, USA.
*Corresponding author: Vinay Saggar
Emergency Medicine, Columbia University College of Physicians and Surgeons, New York, USA.
Email ID: [email protected]
Received: Jun 17, 2025
Accepted: Jul 09, 2025
Published Online: Jul 16, 2025
Journal: Annals of Cardiology
Copyright: Saggar V et al. © All rights are reserved
Citation: Moskovitz K, Saggar V, Giordano JA. An interesting case of an isolated posterior MI from both complete right coronary and left circumflex artery occlusions. Ann Cardiol. 2025; 1(2): 1009.
Background: ST-Elevation Myocardial Infarctions (STEMIs) are one of the most critically assessed cardiovascular pathologies. While anterior and inferior STEMIs present on EKG with appropriate findings of ST-elevation, posterior STEMIs can be more subtle, resulting in a delay of treatment and suboptimal management. This case is an example of a rare isolated posterior MI, with prompt recognition, improvement in the ischemic EKG findings, and good outcome after emergent revascularization.
Case report: 58-year-old male with a history of coronary artery disease was brought in for chest pain. An electrocardiogram was done that showed marked ST-segement depressions from V2-V4 as well as an R/S ratio >1 in V3/V4. Given clinical picture a STEMI notification was activated for concern of posterior MI. Patient was taken to the catheterization lab where he was found to have triple vessel disease including acute thrombotic lesion with 100% occlusion in the proximal Lcx, chronic complete total occlusion of the right coronary artery that led to a baseline left to right collateral system, and 80% stenosis of the left anterior descending. Patient received 2 stents, started on goal-directed medical therapy, and had repeat EKGs showing resolution of ischemic changes.
Discussion: Isolated posterior myocardial infarctions--which account for 4% of all AMIs--are associated with longer door-to-balloon times and worse outcomes because they are frequently missed/delayed in diagnosis. The primary challenge is the lack of ST segment elevation on electrocardiogram) as well as differentiating from sub-endocardial ischemia. Thus, increased awareness of the diagnostic criteria can significantly enhance timely diagnosis and patient prognosis.
Keywords: Posterior MI; STEMI; EKG; Posterior leads; Cardiac catheterization; Chest pain.
ST-Elevation Myocardial Infarctions (STEMIs) are one of the most critically assessed cardiovascular pathologies. With over 900,000 reported cases annually in the United States, STEMIs contribute significantly to cardiovascular morbidity and mortality. They are a subtype of acute coronary syndrome defined by occlusion of coronary arteries resulting in myocardial damage and ischemia [1].
Outcomes in STEMIs are often dependent on the timing of reperfusion therapy [2], which underscores the importance of a prompt diagnosis. While anterior and inferior STEMIs present on EKG with appropriate findings of ST-elevation, posterior STEMIs can be more subtle, resulting in a delay of treatment and suboptimal management [3]. More often than not, posterior STEMI’s usually occur in conjunction with inferior or lateral occlusions [4]. However, approximately 4% of all STEMIs are isolated posterior wall infarcts [4]. The difficulty in identifying an isolated posterior STEMI originates from the limitations of standard 12 lead EKGs which focus on the anterior, inferior, and lateral myocardial walls. The posterior wall’s status can be extrapolated from reciprocal wall changes, often from anterior precordial lead (V1-V4) horizontal ST depressions, rather than the traditional elevation [5]. Additional EKG trends in posterior STEMIs include both an increased R-wave amplitude with upright T waves in leads V1, V2, V3 and an R/S ratio of more than one in V2 [6]. Incorporation of a 15 lead EKG which includes V7, V8, V9 placed on the posterior chest wall can improve sensitivity (66.1%) and positive predictive value (96.8%) in diagnosing posterior myocardial infarctions [7], where ST segment elevations are then looked for in those leads. Similarly, the use high sensitivity troponin or point of care cardiac ultrasound can be used in adjuncts in aid in this difficult diagnosis [8].
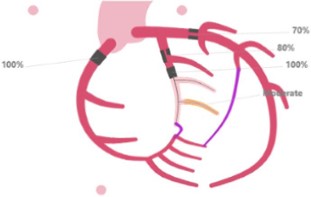
The unique coronary vascular anatomy also impacts the presentation of posterior myocardial infarctions. The posterior walls are primary vascularized by the Posterior Descending Artery (PDA) whose origin arises off either the Right Coronary Artery (RCA) or the Left Circumflex artery (LCx). Approximately 70% of the population are “right dominant” with the PDA originating off the RCA; 10% are “left dominant” with the PDA originating from the LCx, and 20% are codominant with dual RCA and LCx supply [9]. This anatomical distinction has critical implications for EKG interpretation and clinical management, as right-dominant PDA infarctions often present concurrently with inferior STEMIs, whereas left-dominant PDA occlusions can more frequently manifest as isolated posterior MIs due to LCx occlusion [10]. Understanding these anatomical nuances is paramount in tailoring appropriate revascularization strategies and optimizing patient outcomes.
We present a case of a patient presenting with chest pain and concerning features of acute coronary syndrome found to have a posterior STEMI on coronary angiography. This presentation aims to show the importance of considering posterior STEMIs in patients with no active ST elevation on EKG, and highlights this can’t miss diagnosis that still affects tens of thousands of patients a year [10].
Patient was a 58 y/o male with a past medical history of coronary artery disease s/p stents in 2012, tobacco use disorder, and hypertension, who was brought in by EMS for chest pain. The patient was in his usual state of health until an hour prior to arrival, when he began experiencing substernal, exertional chest pain that radiated down his left arm. Patient states he took a baby aspirin with minimal relief and began developing diaphoresis, after which he called EMS. Per EMS, en route, he was given three additional doses of baby aspirin with good response.
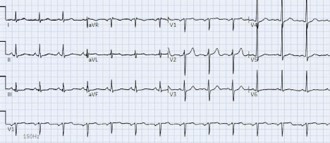
On initial presentation to the Emergency Department, the patient was noted to be hemodynamically stable but diaphoretic and uncomfortable appearing. An immediate electrocardiogram was done (Figure 1) that showed a normal sinus rhythm with marked ST-segement depressions from V2-V4 that progressively worsened and an R/S ratio >1 in V3/V4. Patient had a subsequent posterior EKG done (Figure 2) which did not show overt ST-segment elevations in the posterior leads V7-V9 but given symptoms, comorbidities, and EKG, a STEMI notification was activated.
Cardiology evaluated the patient at bedside and agreed with the need for emergent cardiac catheterization. Patient was started on heparin in the ED, given 1 dose of sublingual nitroglycerine for active chest pain, and taken to the cath lab where he was found to have triple vessel disease (Figure 3) including acute thrombotic lesion with 100% occlusion in the proximal Lcx, chronic complete total occlusion of the right coronary artery that lead to a baseline left to right collateral system, and 80% stenosis of the left anterior descending. Patient recieved 2 DES to the mid-Lcx, but the procedure was complicated by hypotension which required balloon inflation and vasopressors, so the residual OM, distal RCA, and mLAD were left to staging procedure 3-4 weeks later.
The patient was initially transferred to the CCU post-procedure where his workup continued, including a TEE post-cath that showed an ejection fraction of 45-50% and signs of inferobasal hypokinesis. Patient had blood work done all of which were within normal limits (cardiac enzymes were not drawn/ trended), was started on goal-directed medical therapy which he tolerated well, had repeat EKGs done that showed the resolution of ischemic changes (Figure 4), and was eventually safely discharged three days into hospitalization with close cards follow up.


This case is an interesting example of an isolated posterior myocardial infarction a rare type of Acute Myocardial Infarction (AMI), accounting for only about 4% of all AMI’s. Isolated posterior myocardial infarctions are associated with longer door-to-balloon times and worse outcomes because they are frequently missed/delayed in diagnosis. The primary challenge in diagnosing isolated posterior myocardial infarction is the lack of ST segment elevation on electrocardiogram (which is typically seen when associated with inferior and/or lateral wall infarctions) as well as differentiating from sub-endocardial ischemia.
The American College of Cardiology updated their guidance on the evaluation and disposition of acute chest pain in the Emergency Department in 2022, highlighting STEMI equivalents, including posterior MI [11]. They utilize the following criteria for the diagnosis of posterior MI:
1. Horizontal ST-segment depression in V1-V3
2. Dominant R-wave (R/S ratio > 1) in V2
3. Upright T waves in anterior leads
4. Prominent and broad R-wave (>30 ms)
These findings can be confirmed by ST-segment elevation of ≥0.5 mm in at least one of the posterior leads V7-V9. While the above criteria should suggest posterior MI, not all criteria must be met to make the diagnosis. For example, the dominant Rwave in V2 is akin to a q-wave, and may only be seen later in the course of the MI.
Elucidating between posterior MI and subendocardial ischemia has also added to the diagnostic challenges. Myers et al have shown that ST-depression that is maximal in V1-V4 vs V5V6 and the high lateral leads is specific for posterior MI [12].
The initial EKG for this patient (Figure 1) shows a normal sinus rhythm with a heart rate of 84 bpm. There is a normal axis and normal intervals. There is ST-depression with associated upright T-waves noted in leads V2-V5, as well as an R/S ratio >1 in V3/V4. The ST-depression is maximal in leads V3/V4. These findings are consistent with posterior MI, particularly in the setting of clinical symptoms consistent with acute coronary syndrome.
The patient’s cardiac catheterization showed multi-vessel disease, with a 100% acute thrombotic occlusion of the left circumflex artery (Figure 3). Post catheterization and stenting, revascularization can be seen on the patient’s EKG, with near resolution of the previously seen ischemic changes (Figure 4).
This case is an example of a rare isolated posterior MI, with prompt recognition, improvement in the ischemic EKG findings, and good outcome after emergent revascularization. Posterior MI remains an underdiagnosed entity, leading to delayed treatment and worse outcomes compared to other acute MI’s. Increased awareness of the diagnostic criteria can significantly enhance timely diagnosis and patient prognosis.
• Posterior STEMI is often underdiagnosed
Isolated posterior Myocardial Infarction (MI) accounts for only about 4% of all acute MIs and is frequently missed due to the lack of ST-elevation on a standard 12-lead EKG. Instead, it presents with ST-segment depression in V1-V4, making early recognition critical for timely treatment.
• Diagnostic criteria for posterior MI
Horizontal ST-segment depression in V1-V3 Dominant R-wave (R/S ratio >1) in V2
Upright T waves in anterior leads
ST-elevation ≥0.5 mm in posterior leads V7-V9 (if recorded)
• Importance of rapid reperfusion
Early identification and activation of STEMI protocols are crucial, as posterior MI is associated with longer door-to-balloon times and worse outcomes. In this case, emergent cardiac catheterization led to successful revascularization, highlighting the importance of timely intervention.
