-
Email [email protected]
-
Address 848 N. Rainbow Blvd. #5486 Las Vegas, NV 89107, USA
1Department of Internal Medicine, Mayo Clinic, Phoenix, Arizona, USA.
2Department of Cardiovascular Medicine, Mayo Clinic, Phoenix, Arizona, USA.
3Alfaisal University College of Medicine, Riyadh, Saudi Arabia.
4Department of Cardiovascular Surgery, Mayo Clinic, Phoenix, Arizona, USA.
5Department of Cardiovascular Medicine, Mayo Clinic, Rochester, Minnesota, USA.
*Corresponding author: Hesham M Abdalla
Department of Internal Medicine, Mayo Clinic, Phoenix, Arizona, USA.
Email ID: [email protected]
Received: Jun 23, 2025
Accepted: Jul 11, 2025
Published Online: Jul 18, 2025
Journal: Annals of Cardiology
Copyright: Hesham MA et al. © All rights are reserved
Citation: Abdalla HM, Pathangey G, Raslan MA, Downey FX, Majdalany DS. Massive left atrial thrombus: The role of early surgical intervention. Ann Cardiol. 2025; 1(2): 1010.
We present a case of a 40-year-old woman with prior mechanical mitral valve replacement and atrial fibrillation who was found to have a massive left atrial thrombus measuring 12 cm, complicated by ventricular tachycardia. Urgent surgical excision revealed a large nonadherent thrombus with preserved valve function. To our knowledge, this is the largest LA thrombus reported to date and highlights the value of early imaging and multidisciplinary decision-making.
Keywords: Left atrial thrombus; Surgical thrombus excision; Multimodal imaging; Dilated cardiomyopathy; Large atrial mass.
A 40-year-old female with history of mechanical mitral valve replacement, tricuspid annuloplasty, dilated cardiomyopathy, permanent Atrial Fibrillation (AFib), and prior septic cardioembolic stroke presented to a rural facility with fever and dyspnea, reporting warfarin nonadherence. Initial diagnostics showed subtherapeutic INR 1.1, normal hs-Troponin-T and beta-natriuretic peptide levels, and EKG indicating AFib without ischemic changes. Chest CT revealed large Left Atrial (LA) mass measuring 3.9×12.0×8.8 cm. She subsequently developed sustained monomorphic Ventricular Tachycardia (VT) requiring amiodarone infusion. Empiric antibiotics were started for possible endocarditis, and she was transferred on intravenous heparin and amiodarone.
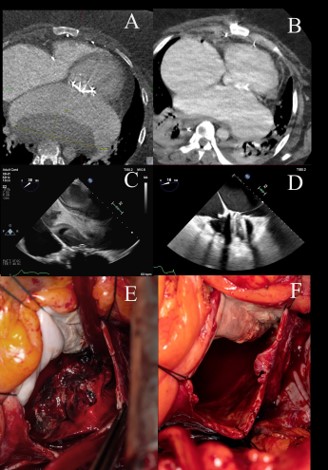
On arrival, recurrent VT was terminated with additional amiodarone boluses. CT confirmed LA mass compressing the esophagus and descending aorta (Figure 1A). Following multidisciplinary consultation, she consented to surgical excision via redo median sternotomy, entering the left atrium just anterior to the left pulmonary veins. Preoperative Transesophageal Echocardiography (TEE) showed preserved left ventricular ejection fraction (60%), biatrial enlargement, and large echodensity in posterior LA (Figure 1D). Intraoperatively, substantial nonadherent thrombus was excised (Figures 1B & 1C). Remarkably, the mechanical valve remained free of thrombus and continued to function optimally. Admitting blood cultures remained negative. She was discharged on postoperative day 30 on warfarin (Figure 1E).
To our knowledge, this case represents the largest LA mass documented in the literature. Management of large atrial thrombi presents significant challenges due to the lack of definitive guidelines for size classification and treatment strategies. Further research to guide management decisions on surgical excision versus prolonged anticoagulation.
Funding: The authors declare that no external funding was received for the research, authorship, or publication of this article.
Conflict of interest:The authors declare that they have no conflicts of interest related to this publication. No financial, personal, or professional affiliations have influenced the work presented in this manuscript.
Supplementary material
Video 1: Cine loop demonstrating a large thrombus within the left atrium, delineated by surrounding echocontrast.
Video 2: Cine loop illustrating marked cardiomegaly with a significantly enlarged left atrium. A sizable left atrial mass is visualized exerting compressive effects on the esophagus and descending aorta.
