-
Email [email protected]
-
Address 848 N. Rainbow Blvd. #5486 Las Vegas, NV 89107, USA
1Ukonga Prisons General Hospital, Tanzania Prison Service, Tanzania.
2Department of Internal Medicine, Weill Bugando School of Medicine, Catholic University of Health and Allied Sciences, Tanzania.
*Corresponding author: Asha Mangara
Ukonga Prisons General Hospital, Tanzania Prison Service. P.O. Box 18021, Dar-es-salaam, Tanzania.
Email ID: [email protected]
Received: Aug 28, 2025
Accepted: Sep 29, 2025
Published Online: Oct 05, 2025
Journal: Annals of Cardiology
Copyright: Mangara A. © All rights are reserved
Citation: Mangara A, Kalokola F. Association between diabetes mellitus and coronary slow flow phenomenon. Ann Cardiol. 2025; 1(2): 1011.
Background: Coronary Slow Flow Phenomenon (CSFP) is an angiographic finding characterized by delayed distal vessel opacification without significant epicardial coronary disease. Despite a generally favorable prognosis, CSFP is associated with serious cardiac events, including myocardial infarction and sudden cardiac death, significantly impacting quality of life. Its pathophysiological mechanisms and clinical implications remain poorly understood. The aim of this study was to investigate the association between Diabetes Mellitus (DM) and CSFP. Methodology: This cross-sectional study included 200 patients undergoing coronary angiography for suspected or diagnosed coronary artery disease at the First Affiliated Hospital of Zhengzhou University. Patients were divided into diabetic (n=100) and non-diabetic (n=100) groups. Coronary flow was assessed using the Thrombolysis in Myocardial Infarction (TIMI) frame count (TFC) method, with subgroups classified as normal or slow flow. Sociodemographic, laboratory, and clinical data were extracted from hospital records. Statistical analyses, including chi-square tests and multivariate regression, were performed using SPSS 21.0. Results: CSFP was more prevalent in the diabetic group (39/58, 67.2%) than in the nondiabetic group (19/58, 32.8%), with a statistically significant association (χ²=9.71, df=1, P=0.002). A positive correlation was observed between DM and CSFP (r=0.22, P=0.0001). CSFP was also significantly correlated with male gender (r=0.15, P=0.035), random blood glucose (RBG) levels (r=0.17, P=0.016), hematocrit (r=0.14, P=0.04), hemoglobin (r=0.15, P=0.04), Red cell Distribution Width (RDW) (r=0.14, P=0.04), and B-type Natriuretic Peptide (BNP) (r=0.153, P=0.03). Conclusion: Diabetes Mellitus (DM) is significantly associated with the Coronary Slow Flow Phenomenon (CSFP) and may serve as an independent risk factor. These findings highlight the need for routine diabetes screening and optimal glycemic control in patients with suspected coronary artery disease, as early identification and management may help reduce CSFP-related adverse cardiovascular events.
Keywords: Coronary slow flow phenomenon; Diabetes mellitus; Coronary artery disease; Coronary angiography; TIMI frame count.
The Coronary Slow Flow Phenomenon (CSFP) is an angiographic observation characterized by delayed opacification of the distal coronary vasculature during coronary angiography, despite the absence of significant epicardial coronary artery obstruction [1]. First described by Tambe et al. in 1972, CSFP is identified using the Thrombolysis In Myocardial Infarction (TIMI) frame count (TFC) method, which quantifies the number of cine-angiographic frames required for contrast to reach distal coronary landmarks [2]. Normal TFC values are approximately 36±3 for the Left Anterior Descending artery (LAD, corrected to 21±2), 22±4 for the Left Circumflex Artery (LCX), and 20±3 for the Right Coronary Artery (RCA), with values exceeding these indicatives of slow flow [2]. Clinically, CSFP manifests with a diverse spectrum of presentations including stable or unstable angina, Non-ST-Elevation Myocardial Infarction (NSTEMI), ST-Elevation Myocardial Infarction (STEMI), and Non-Sustained Ventricular Tachycardia (NSVT) [3]. Patients with CSFP often experience recurrent chest pain, which can significantly impair quality of life [4]. Despite its generally favorable prognosis, CSFP has been associated with severe cardiac events, such as acute myocardial infarction, sudden cardiac death, cardiac dysfunction, and fatal arrhythmias [5]. The pathophysiological mechanisms underlying CSFP remain poorly elucidated, but proposed contributors include microvascular dysfunction, endothelial impairment, and inflammatory processes [6]. These uncertainties underscore the need for further research to clarify CSFP’s clinical implications and risk factors, particularly in populations with comorbidities known to exacerbate vascular pathology.
Diabetes Mellitus (DM) is a well-established risk factor for Coronary Artery Disease (CAD), contributing to both macrovascular and microvascular complications through mechanisms such as endothelial dysfunction, oxidative stress, and prothrombotic states [7]. DM affects vascular function by impairing Nitric Oxide (NO) bioavailability and increasing endothelin-1 production, which disrupts the balance necessary for vasodilation and promotes vasoconstriction [8]. This vascular dysfunction is particularly relevant in the context of CSFP, as it may exacerbate microvascular resistance and impair coronary blood flow [9]. Studies have shown that DM is associated with higher rates of cardiovascular morbidity and mortality, even in the absence of obstructive CAD, suggesting that microvascular abnormalities may precede overt atherosclerosis [10]. In patients with CSFP, DM has been linked to increased prevalence of metabolic syndrome, elevated low-density lipoprotein levels, and higher body mass index, all of which compound cardiovascular risk [11]. Furthermore, hyperglycemia, a hallmark of DM, is implicated in creating a prothrombotic and inflammatory environment that may contribute to the pathogenesis of CSFP [12]. The chronic nature of DM-related vascular changes, including capillary microaneurysms and impaired blood flow leading to tissue ischemia, highlights its potential role as a key determinant of CSFP [13]. However, the precise relationship between DM and CSFP remains underexplored, with limited data on whether DM acts as an independent risk factor or merely exacerbates other predisposing conditions. The interplay between DM and CSFP is of particular interest given the rising global prevalence of DM and its associated cardiovascular burden [14]. Emerging evidence suggests that DM-induced microvascular dysfunction may serve as an early marker of coronary vascular pathology, potentially identifiable through angiographic findings like CSFP [15]. Previous studies, such as those by Emrah et al. (2006) and Shuang et al. (2011), have reported associations between DM and CSFP, with mechanisms including reduced NO synthase activity, platelet activation abnormalities, and atherosclerosis-independent microvascular impairments [16,17]. These findings suggest that DM may not only increase the likelihood of CSFP but also amplify its clinical consequences, such as recurrent angina and acute coronary events [18]. Additionally, CSFP’s association with other risk factors, such as male gender, elevated glucose levels, and hematological markers like hematocrit and red cell distribution width, points to a multifactorial etiology where DM plays a central role [19]. Understanding this relationship is critical for developing targeted screening and management strategies for patients with CAD or suspected CAD, particularly those with DM. This study seeks to address the gap in knowledge by investigating whether DM is independently associated with CSFP, thereby providing insights that could guide clinical practice in preventing and managing this underrecognized phenomenon.
Study design and population
This cross-sectional study was conducted at the Department of Cardiology, First Affiliated Hospital of Zhengzhou University, Henan Province, P.R. China. A total of 200 patients with suspected or diagnosed coronary artery disease undergoing coronary angiography were enrolled. Patients were divided into two groups: diabetic (n=100) and non-diabetic (control, n=100). Each group was further subdivided into normal flow and slow flow subgroups based on TIMI Frame Count (TFC) assessments.
Inclusion and exclusion criteria
Inclusion criteria: Patients with suspected or diagnosed coronary artery disease and no prior history of Percutaneous Coronary Intervention (PCI).
Exclusion criteria: Coronary lesions >50%, prior PCI, or incomplete data.
Coronary angiography and TIMI frame count
Coronary angiography was performed via the percutaneous transradial approach using the Judkins technique, with images acquired at 30 frames/second. Two trained cardiologists analyzed the angiograms, defining normal coronary arteries as those without visible atherosclerosis, thrombosis, or spasm. Obstructive coronary lesion was defined as that compromising the luminal diameter by 50% or more. TFC was measured as described by Gibson et al. [6]. The initial frame was defined when contrast occupied ≥70% of the proximal coronary lumen, and the final frame was when contrast reached the distal landmark (distal bifurcation for Left Anterior Descending artery [LAD], distal bifurcation of longest segment for Left Circumflex artery [LCX] and first posterolateral branch for Right Coronary Artery [RCA]). LAD TFC was corrected (cTFC) by dividing by 1.7. Normal TFC values were: LAD, 36±3 (cTFC 21±2); LCX, 22±4; RCA, 20±3. Values exceeding these were classified as slow flow.
Data collection
Sociodemographic characteristics, clinical presentation details, and laboratory investigation results including Random Blood Glucose (RBG), glycated Hemoglobin (HbA1c), hematocrit, hemoglobin, Red cell Distribution Width (RDW), B-type Natriuretic Peptide (BNP), troponin, and Creatine Kinase-MB (CKMB) were retrieved from the hospital information system. All data were anonymized prior to analysis to ensure confidentiality.
Statistical analysis
Data were analyzed using SPSS 21.0. Numerical variables were compared using Student’s t-test, and categorical variables were assessed with chi-square tests. Correlations were evaluated using Pearson’s (numerical) and Spearman’s (categorical) tests. Multivariate logistic regression adjusted for confounders. A P-value <0.05 was considered statistically significant.
Results
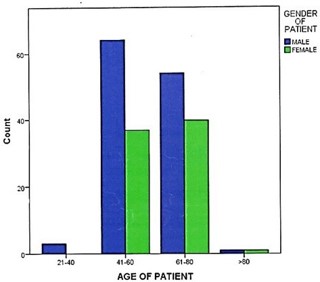
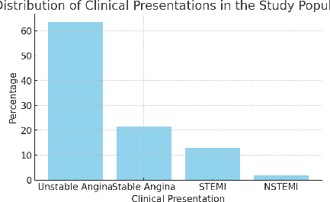
This cross-sectional study enrolled 200 patients, equally divided into diabetic (n=100) and non-diabetic (n=100) groups, with no gender differentiation. The participants’ ages ranged from 23 to 81 years (Figure 1). Overall, the cohort comprised 122 males (61%) and 78 females (39%) Clinical presentations included unstable angina (127, 63.5%), stable angina (43, 21.5%), ST-elevation myocardial infarction (STEMI; 26, 13%), and NonST-Elevation Myocardial Infarction (NSTEMI; 4, 2%) (Table 1) (Figure 2). Coronary flow assessment using the TIMI Frame Count (TFC) method revealed normal coronary flow in 142 (71%) patients and Coronary Slow Flow Phenomenon (CSFP) in 58 (29%) patients (Figure 3). Among CSFP patients, slow flow was observed in the left circumflex artery (LCX; 42/58, 72.4%), right coronary artery (RCA; 32/58, 55.2%), and Left Anterior Descending artery (LAD; 9/58, 15.5%) Single-vessel slow flow was noted in 36 patients, two-vessel in 19, and three-vessel in 3 (Table 2).
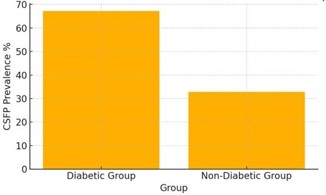
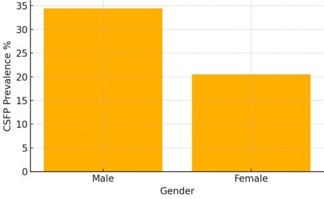
CSFP was significantly more prevalent in the diabetic group (39/58, 67.2%) compared to the non-diabetic group (19/58, 32.8%), with a chi-square test indicating statistical significance (χ²=9.71, df=1, P=0.002) (Figure 4). A positive correlation was observed between Diabetes Mellitus (DM) and CSFP (r=0.22, P=0.0001). Male gender was also significantly associated with CSFP (r=0.15, P=0.035), with 42/58 (72.4%) CSFP patients being male compared to 16/58 (27.6%) female (Figure 5). Within genders, the proportion of CSFP was higher in males (34.4%) than females (20.5%) (χ²=4.47, df=1, P=0.03). Other significant correlations with CSFP included random blood glucose levels (RBG; r=0.17, P=0.016), hematocrit (r=0.14, P=0.04), hemoglobin (r=0.15, P=0.04), Red cell Distribution Width (RDW; r=0.14, P=0.04), and B-type natriuretic peptide (BNP; r=0.153, P=0.03) (Table 3).
HbA1c levels were significantly higher in the diabetic group (7.44±1.44 vs. 5.79±0.43, P=0.001) and correlated with DM (r=0.622, P=0.0001). In CSFP patients, HbA1c was higher compared to those with normal flow (6.81±1.17 vs. 6.63±1.47), but the correlation with CSFP was not statistically significant (P>0.05). Other biochemical parameters showed no significant association with CSFP (P>0.05) (Table 4).
| Characteristic n (%) | Total (n=200) | Diabetic Group (n=100) | Non-Diabetic Group (n=100) |
|---|---|---|---|
| Male | 122(61%) | 61(61%) | 61(61%) |
| Female | 78(39%) | 39(39%) | 39(39%) |
| Clinical presentation | |||
| Unstable Angina | 127(63.5%) | 64(64%) | 63(63%) |
| Stable Angina | 43(21.5%) | 21(21%) | 22(22%) |
| STEMI | 26(13%) | 13(13%) | 13(13%) |
| NSTEMI | 4(2%) | 2(2%) | 2(2%) |
| Vessel Involvement | Number of patients (n=58) | Percentage (%) |
|---|---|---|
| LAD | 9 | 15.50% |
| LCX | 42 | 72.40% |
| RCA | 32 | 55.20% |
| Single Vessel | 36 | 62.10% |
| Two Vessels | 19 | 32.80% |
| Three Vessels | 3 | 5.20% |
| Parameter | Correlation Coefficient (r) | P-value |
|---|---|---|
| Diabetes Mellitus | 0.22 | 0.0001 |
| Male Gender | 0.15 | 0.035 |
| Glucose Level | 0.17 | 0.016 |
| Hematocrit | 0.14 | 0.04 |
| Hemoglobin | 0.15 | 0.04 |
| RDW | 0.14 | 0.04 |
| BNP | 0.153 | 0.03 |
| Variable | P Value | Variable | P Value |
|---|---|---|---|
| Age | 0.945 | Urea | 0.109 |
| Hypertension | 0.904 | Createnine | 0.117 |
| Troponin T | 0.369 | Uric Acid | 0.573 |
| Smoking Status | 0.146 | HbAlc | 0.398 |
| Drinking Status | 0.124 | Hb | 0.037 |
| Gender | 0.035 | HCT | 0.047 |
| CKMB | 0.393 | RDW | 0.044 |
| BNP | 0.03 | MPV | 0.567 |
| Total Cholesterol | 0.612 | Fibrinogen | 0.94 |
| TG | 0.234 | HsCRP | 0.199 |
| HDL | 0.059 | TFC | 0.001 |
| LDL | 0.57 | TFC.LAD | 0.001 |
| Potassium | 0.942 | CTFC.LAD | 0.001 |
| Sodium | 0.241 | TFCLCX | 0.001 |
| Glucose | 0.016 | TFC.RCA | 0.001 |
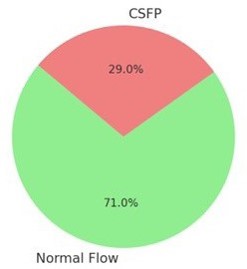
A pie chart showing the prevalence of normal coronary flow (71%) and CSFP (29%).
Our study demonstrates a significant association between Diabetes Mellitus (DM) and the Coronary Slow Flow Phenomenon (CSFP), with a higher prevalence of CSFP in diabetic patients compared to non-diabetic controls, and a positive correlation between glucose levels and CSFP. These findings reinforce prior reports linking DM to CSFP in patients with angiographically normal coronary arteries [8,16,17]. The CSFP prevalence in our cohort is notably higher than the 1-7% reported in most studies [10,17], but aligns with more recent data reporting a prevalence of 34% [11]. This discrepancy may reflect differences in patient populations, diagnostic methods—particularly the use of the TIMI Frame Count (TFC) or regional variations in DM prevalence.
The significant correlation between glucose levels and CSFP highlights hyperglycemia as a key contributor, consistent with studies identifying glucose as an independent predictor of CSFP [14]. These results suggest that DM exacerbates microvascular dysfunction—a critical mechanism in CSFP independent of epicardial coronary artery disease.
The underlying pathophysiology of CSFP in diabetic patients likely involves endothelial dysfunction and impaired microvascular perfusion. This is supported by observed correlations with hematocrit, hemoglobin, Red cell Distribution Width (RDW), and B-type Natriuretic Peptide (BNP). Hyperglycemia disrupts Nitric Oxide (NO) bioavailability and enhances endothelin-1 production, leading to vasoconstriction and reduced coronary blood flow [13]. Additionally, DM promotes a prothrombotic and inflammatory state, which may increase microvascular resistance [12]. The association with hematological markers, as supported by previous studies [20], suggests that increased blood viscosity and systemic inflammation contribute to the development of CSFP.
The higher CSFP prevalence in males is consistent with previous reports suggesting gender-specific differences in vascular reactivity or cardiovascular risk factor burden [19]. Notably, the predominance of Left Circumflex Artery (LCX) involvement among CSFP patients may reflect vessel-specific vulnerabilities due to anatomical or hemodynamic factors, meriting further investigation.
Clinically, these findings underscore the importance of DM as a modifiable risk factor for CSFP, with implications for cardiovascular risk stratification. The high prevalence of CSFP in diabetic patients, coupled with its association with recurrent angina and adverse cardiac events [5], highlights the need for targeted screening during coronary angiography. Interestingly, although HbA1c levels were elevated in CSFP patients, the correlation was not statistically significant contrasting with similar studies [17]. This may reflect variability in glycemic control or study-specific factors. Nevertheless, elevated HbA1c remains a marker of cardiovascular risk and should be closely monitored.
Integrating CSFP assessment into routine coronary angiographic protocols for diabetic patients could facilitate early detection and management, potentially improving outcomes. Furthermore, the observed correlations with RDW and BNP suggest that CSFP may serve as a marker of systemic inflammation and cardiac stress, expanding its diagnostic utility.
The broader implications of this study are substantial, especially given the growing global burden of DM and its cardiovascular complications. By identifying DM as an independent risk factor for CSFP, our findings support a paradigm shift in managing patients with suspected coronary artery disease—emphasizing microvascular assessment alongside traditional epicardial evaluation. The significant glucose–CSFP correlation suggests that tighter glycemic control could reduce the risk of CSFP, aligning with broader evidence on DM management [14].
Future research should investigate whether therapies targeting microvascular dysfunction, such as vasodilators or antiinflammatory agents, can improve clinical outcomes in CSFP patients. Additionally, the gender and vessel-specific patterns observed in this study highlight the potential for personalized approaches to CSFP management tailored to patient demographics and angiographic findings.
This study has several limitations. Its cross-sectional design precludes causal inference, and longitudinal studies are needed to clarify the temporal relationship between DM and CSFP. The single-center nature of the study may limit generalizability, and unmeasured confounding factors such as lifestyle habits or concurrent medications—could have influenced the findings. Moreover, the lack of long-term follow-up data restricts conclusions regarding the prognostic implications of CSFP.
We recommend routine DM screening for patients with suspected or confirmed coronary artery disease, alongside aggressive glycemic control to prevent CSFP and associated cardiac events. Multicenter studies with larger and more diverse populations are essential to validate our findings and explore therapeutic strategies for CSFP in diabetic patients.
This study establishes diabetes mellitus as an independent risk factor for the coronary slow flow phenomenon, with significant correlations between CSFP and glucose levels. Although HbA1c levels were elevated in CSFP patients, their correlation with CSFP was not statistically significant. These findings underscore the need for DM screening and effective glycemic control in patients with coronary artery disease to reduce CSFP-related cardiovascular risks, advocating for enhanced microvascular assessment in clinical practice.
Ethical approval and consent to participate: This study was conducted as part of the requirements for the Master of Clinical Medicine (MMed) in Internal Medicine (Cardiology) Degree at Zhengzhou University, Henan Province, People’s Republic of China, under the academic supervision of Prof. Chun Guang Qiu. Permission to conduct the study was granted by the management of First affiliated hospital of Zhengzhou University. Ethical approval to conduct the research was obtained from the Ethics Committee of Zhengzhou University Registration number 201222500006/10459.
Given that the study involved retrospective analysis of existing clinical and angiographic data routinely collected during patient care, the Ethics Committee granted a waiver of written informed consent. This waiver was provided on the basis that the research posed no more than minimal risk to participants, involved no direct patient contact, and included no identifiable personal information.
All methods were performed in accordance with the ethical principles of the Declaration of Helsinki and relevant national and institutional guidelines and regulations. Strict confidentiality was maintained throughout the study, with data anonymized before analysis and securely stored to prevent unauthorized access.
Availability of data and material: All data generated for this study, including figures and tables, are included in this manuscript.
Conflicts of interest: The authors declare that they have no conflict of interest.
Funding: This research was privately sponsored as part of Asha Mangara’s academic program and did not receive any external financial support.
Author’s contributions: AM designed the study, developed the methodology, and participated in data collection, analysis, interpretation and manuscript development. FK contributed to manuscript development. All authors critically reviewed the manuscript and approved the final version for submission.
Acknowledgements: We express our sincere gratitude to all the patients whose data contributed to this study. We are deeply grateful to Prof. Chun Guang Qiu, whose supervision, guidance, and insightful feedback were invaluable throughout the design, execution, and completion of this research. Special thanks are also extended to the management and staff of the Department of Cardiology, First Affiliated Hospital of Zhengzhou University, for their cooperation and technical support. Finally, we acknowledge the academic and administrative support provided by Zhengzhou University during the course of the Master of Clinical Medicine (MMed) program.
