-
Email [email protected]
-
Address 848 N. Rainbow Blvd. #5486 Las Vegas, NV 89107, USA
1Department of Cardiovascular Medicine, Tan Tock Seng Hospital, National Healthcare Group, Singapore.
2Mount Elizabeth Hospital, Singapore.
3Department of Cardiology, Hurstville Private Hospital, Sydney, Australia.
4Department of Cardiology, Concord Hospital, Sydney, Australia.
5Department of Wellington Cardiology, Wellington Hospital, Wellington, New Zealand.
6Cardiovascular Unit, North Shore Hospital, Auckland, New Zealand.
*Corresponding author: Bharat Khialani
Department of Cardiovascular Medicine, Interventional Cardiologist Tan Tock Seng Hospital, National Healthcare Group, Singapore.
Email ID: [email protected]
Received: Dec 05, 2025
Accepted: Jan 05, 2026
Published Online: Jan 12, 2026
Journal: Annals of Cardiology
Copyright: Khialani B et al. © All rights are reserved
Citation: Yar D, Haan LI, Yi PR, Francis PJ, Khialani B, et al. Myocardial infarction secondary to significant myocardial bridging: A case report with multimodality imaging correlation. Ann Cardiol. 2026; 3(1): 1014.
Myocardial Bridging (MB) is a congenital anomaly in which a segment of an epicardial coronary artery courses intramurally through the myocardium. Although often considered benign, MB can rarely lead to Acute Coronary Syndromes (ACS) including myocardial infarction. We report a case of a 56-yearold man presenting with ST-Elevation Myocardial Infarction (STEMI) caused by MB of the mid Left Anterior Descending (LAD) artery. Coronary angiography revealed dynamic systolic compression (“milking effect”) of the LAD without atherosclerotic stenosis. Administration of intracoronary nitrates aggravated compression, while beta-blocker therapy alleviated ischemic changes. Coronary Computed Tomography Angiography (CCTA) confirmed a 20 mm tunnelled segment with >70% systolic narrowing. Cardiac Magnetic Resonance (CMR) imaging demonstrated late gadolinium enhancement consistent with infarction in the LAD territory. The patient was managed conservatively with nondihydropyridine calcium channel-blockers, with resolution of symptoms at 6-month follow-up. This case highlights the importance of multimodality imaging for diagnosis and functional assessment of MB, and underscores that MB, though frequently incidental, can cause clinically significant myocardial ischemia and infarction.
Keywords: Myocardial bridging; Acute coronary syndrome; ST-elevation myocardial infarction; Coronary angiography; Multimodality imaging.
Myocardial Bridging (MB) is a congenital coronary anomaly in which a segment of an epicardial coronary artery, most commonly the Left Anterior Descending artery (LAD), takes an intramural course within the myocardium rather than following the usual epicardial trajectory. During systole, the bridged segment undergoes dynamic compression, producing the characteristic angiographic “milking effect.” The reported prevalence of MB varies widely depending on the diagnostic modality, ranging from 5-15% on invasive coronary angiography to over 40% in autopsy and Coronary Computed Tomography Angiography (CCTA) studies [1-3].
While often regarded as a benign incidental finding, MB has been increasingly recognized as a potential cause of myocardial ischemia, arrhythmias, syncope, and even sudden cardiac death [2,4,5]. Its pathophysiological significance arises from both mechanical and endothelial mechanisms: systolic compression, delayed diastolic relaxation, endothelial dysfunction, altered shear stress, and vasospasm, all of which can impair coronary flow and promote atherosclerosis proximal to the bridged segment [6-9]. In rare instances, these processes can precipitate Acute Coronary Syndromes (ACS) in the absence of fixed obstructive disease.
Acute Myocardial Infarction (MI) secondary to MB is uncommon but clinically relevant, as its recognition alters management. Several reports have described MB-related unstable angina, NSTEMI, and STEMI presentations [10-13]. Therapeutic strategies differ fundamentally from those used in atherosclerotic coronary artery disease: beta-blockers and calcium channel blockers are preferred for symptom control, whereas nitrates are contraindicated due to exacerbation of systolic compression [4,5,14]. In selected refractory or high-risk cases, invasive or surgical interventions such as stent implantation, myotomy, or coronary bypass may be considered.
In this review, we discuss the contemporary understanding of myocardial bridging, focusing on its clinical implications, diagnostic evaluation, and therapeutic approaches. To illustrate these principles, we present a representative case of STSegment Elevation Myocardial Infarction (STEMI) caused by a hemodynamically significant mid-LAD bridge in the absence of atherosclerotic disease, comprehensively assessed using multimodality imaging.
A 56-year-old man presented with acute substernal chest pain radiating to the left arm. The pain occurred at rest, was severe, and associated with diaphoresis. He was a current smoker but had no other cardiovascular risk factors. On arrival, he was hemodynamically stable. Physical examination was unremarkable.
Electrocardiogram (ECG) revealed 1 mm ST-segment elevation with T-wave inversions in leads V2-V6 (Figure 1A). High-sensitivity troponin T was elevated to 2631 ng/L (reference <14 ng/L). A diagnosis of anterior STEMI was made, and the patient was referred for urgent coronary angiography.

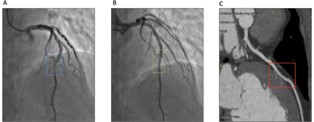
Coronary angiography demonstrated dynamic systolic compression of the mid-LAD with near-total narrowing in systole and resolution in diastole, consistent with MB (Figures 2A & 2B). No fixed stenosis or significant atherosclerotic plaques were identified in any vessel. CCTA was then performed to delineate anatomy. It demonstrated a 12 mm tunnelled segment in the mid-LAD with mild 50% luminal narrowing in diastole, without calcified or non-calcified plaques (Figure 2C). Such anatomical characterization has been shown to improve diagnostic yield compared with angiography alone [7,8].
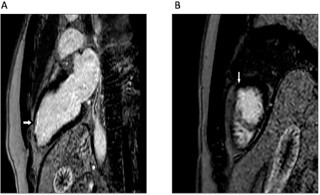
Cardiac Magnetic Resonance imaging (CMR) was obtained for functional assessment. Resting images demonstrated a subendocardial defect in the LAD territory, while late gadolinium enhancement confirmed infarction (Figures 3A & 3B). Left ventricular systolic function was preserved (ejection fraction 58%). CMR is particularly valuable in confirming ischemia and tissue injury in MB-related ACS [4,15].
The patient was treated conservatively with nondihydropyridine calcium channel blockers. Nitrates were strictly avoided. Statin therapy was initiated for better lipid control, and he was counselled on smoking cessation. At 6-month followup, he was asymptomatic, with normalized ECG (Figure 5) and serum troponin levels. No repeat imaging was performed given clinical stability.

Pathophysiology of MB
While angiography highlights systolic compression, ischemia in MB is largely mediated by impaired diastolic perfusion, particularly during tachycardia, when diastolic filling is shortened [9,16]. Histopathology studies have demonstrated intimal thickening, smooth muscle hyperplasia, and endothelial dysfunction within bridged segments, contributing to vasomotor abnormalities [10,11]. Additionally, altered wall shear stress predisposes to atherosclerosis proximal to the MB [6,11], though this was not seen in our patient.
MB and acute coronary syndromes
Although MB is generally considered a benign anatomical variant, multiple reports confirm its potential to precipitate ACS, including STEMI, particularly when the depth or length of the tunneled segment results in significant systolic compression [12,13,17]. Several pathophysiological mechanisms have been proposed. These include dynamic supply–demand mismatch due to tachycardia or heightened contractility, endothelial dysfunction with superimposed vasospasm, microvascular impairment limiting diastolic perfusion, and in cases with concomitant atherosclerosis, plaque rupture proximal to the bridged segment, where abnormal shear forces tend to promote plaque formation.
Our case is unusual in that infarction occurred despite the absence of angiographic or intravascular evidence of atherosclerotic plaque. Nonetheless, cardiac MRI demonstrated clear myocardial necrosis within the LAD territory, suggesting that MB alone, through severe dynamic compression and its downstream effects on perfusion and microvascular integrity, can in rare circumstances be sufficient to trigger transmural infarction.
Diagnostic role of multimodality imaging
Angiography remains the gold standard, showing the “milking effect” [3]. However, angiography underestimates depth and length. CCTA provides superior anatomical definition, identifying the extent of tunnelling and excluding concomitant atherosclerosis [7,8]. Intravascular Ultrasound (IVUS) and Optical Coherence Tomography (OCT) can delineate vessel wall morphology and confirm systolic compression [16]. Functional assessment with Instantaneous wave-Free Ratio (iFR) or dobutamine Fractional Flow Reserve (FFR) has also been applied to MB, to evaluate hemodynamic significance [18]. Finally, CMR provides unique value in detecting ischemia and infarction [15]. Our patient benefitted from both CCTA and CMR, enabling precise correlation between anatomy and functional impact.
Therapeutic approaches
First-line therapy for symptomatic MB generally consists of rate-limiting agents, such as beta-blockers or non-dihydropyridine calcium channel-blockers. These medications reduce heart rate and contractility, which helps prolong the diastolic filling time and diminish the degree of systolic compression of the bridged artery [2,4,5]. In contrast, nitrates are contraindicated for MB patients because they can increase vessel compliance and worsen the compression during systole, thereby enhancing systolic narrowing and potentially exacerbating symptoms or causing more severe conditions [2,5,15].
There are case series of effective Percutaneous Coronary Intervention (PCI) for MB [14,16], although this is associated with high rates of restenosis, stent fracture, and thrombosis, limiting its role. Surgical myotomy or Coronary Artery Bypass Grafting (CABG) are options for refractory cases with severe ischemia [4,5]. Our patient responded well to calcium channel blockers, obviating the need for invasive or surgical therapy. The various therapeutic options for management of symptomatic MB are summarised in (Table 1).
| Therapy | Role/Indication | Rationale/Notes |
|---|---|---|
| Beta-blockers (First-line) | Symptomatic MB | Reduce heart rate and contractility → prolong diastole → lessen systolic compression of the bridged segment. |
| Non-dihydropyridine calcium channel blockers (e.g., diltiazem, verapamil) | Alternative or adjunct first-line therapy | Similar hemodynamic effect as beta-blockers; helpful when vasospasm coexists. |
| Nitrates | Contraindicated | Increase vessel compliance → worsen systolic compression → may exacerbate symptoms or cause severe hemodynamic worsening. |
| PCI (stenting) | Not routinely recommended; limited role | High rates of restenosis, stent fracture, and thrombosis; mechanical forces from the bridged segment compromise stent integrity. |
| Surgical myotomy | Refractory symptoms with documented ischemia | Directly relieves systolic compression by unroofing the tunnelled segment. |
| CABG | Selected refractory cases (especially deep bridges or long segments) | Bypass grafting avoids the mechanically compressed segment; used when myotomy is unsuitable. |
Prognosis
Most MB patients, including those with ischemic presentations, have a favourable prognosis when managed appropriately. Long-term outcomes hinge on symptom control, risk factor modification, and avoidance of inappropriate therapies (e.g., nitrates). Smoking cessation was particularly emphasized in this case, as it is a risk factor for recurrence.
This case highlights myocardial bridging as a rare cause of STEMI in the absence of atherosclerosis. Multimodality imaging, including angiography, CCTA, and CMR, was crucial in confirming diagnosis, delineating anatomy, and establishing functional significance. Calcium channel-blocker therapy proved effective, and cardiovascular risk factors were optimised. Clinicians should recognize MB as a potential mechanism of ACS and tailor management accordingly.
