-
Email [email protected]
-
Address 848 N. Rainbow Blvd. #5486 Las Vegas, NV 89107, USA
1Department of Cardiovascular Medicine, Tan Tock Seng Hospital, National Healthcare Group, Singapore.
2Department of Cardiology, Woodlands Health Campus, National Healthcare Group, Singapore.
3Department of Wellington Cardiology, Wellington Hospital, Wellington, New Zealand.
4Department of Cardiology, Hurstville Private Hospital, Sydney, Australia.
5Department of Cardiology, Concord Hospital, Sydney, Australia.
6Hospital Sultanah Bahiyah, Alor Setar, Malaysia.
7Cardiovascular Unit, North Shore Hospital, Auckland, New Zealand.
*Corresponding author: Bharat Khialani
Department of Cardiovascular Medicine, Interventional Cardiologist, Tan Tock Seng Hospital, National Healthcare Group, Singapore.
Email ID: [email protected]
Received: Dec 07, 2025
Accepted: Jan 09, 2026
Published Online: Jan 16, 2026
Journal: Annals of Cardiology
Copyright: Khialani B et al. © All rights are reserved
Citation: Khialani B, Jun ESW, Shing AA, Khaing T, Fairley S, et al. The fluoroscopic IVUS X-mark IT (FIX-IT) technique: A reproducible, image-guided approach to ostial stent deployment. Ann Cardiol. 2026; 3(1): 1015.
Ostial coronary lesions present significant technical challenges during Percutaneous Coronary Intervention (PCI), where imprecise stent positioning can result in geographic miss, stent protrusion, or compromised future access. Angiographic guidance alone is often limited by vessel foreshortening, overlapping structures, and variable aortic root anatomy. Although Intravascular Ultrasound (IVUS) provides high-resolution visualization of the coronary ostium and plaque morphology, its integration into real-time ostial stent deployment has been inconsistent, partly due to equipment and technical constraints. The Fluoroscopic IVUS X-mark IT (FIXIT) technique offers a simple, reproducible solution by using IVUS to identify the true anatomical ostium and translate this landmark precisely onto fluoroscopy. This facilitates accurate stent placement while minimizing contrast use and reducing the risk of geographic miss. We describe the application of FIX-IT for ostial Left Anterior Descending (LAD) artery stenting across three different IVUS platforms, demonstrating its adaptability, procedural reliability, and potential to improve technical success and longterm outcomes in ostial PCI.
Ostial coronary lesions are a challenging subset of coronary artery disease, requiring precise stent placement at the true vessel origin during PCI [1]. Inaccurate positioning can cause geographic miss or stent protrusion into the parent vessel, impairing flow or complicating future procedures. These challenges are heightened by the limitations of angiographic guidance, which depends on visual estimation and may be unreliable in cases of vessel foreshortening, overlapping anatomy, or complex aortic root structures.
While Intravascular Ultrasound (IVUS) has emerged as a powerful imaging modality to enhance visualization of coronary lesions, its full potential in guiding ostial stent placement remains underutilized in routine clinical practice. IVUS provides high-resolution cross-sectional imaging that enables precise identification of anatomical landmarks such as the vessel ostium, plaque morphology, and optimal landing zones [2]. However, integrating this information into realtime procedural strategy, especially for ostial interventions, requires a systematic approach. Real time IVUS guided stenting is one proposed method allowing accurate ostial stent placement [3], but does require larger guide catheter sizes and smaller profile IVUS catheters.
This report describes the Fluoroscopic IVUS X-mark IT (FIX-IT) technique, a simple and reproducible method that uses intracoronary IVUS to identify and fluoroscopically mark the true anatomical ostium. This enables precise stent placement, minimizes geographic miss, and reduces contrast use. By integrating IVUS data with fluoroscopy, FIX-IT bridges the gap between imaging and execution. We applied the technique using three different IVUS systems, demonstrating its consistency, adaptability, and potential to enhance procedural accuracy and longterm outcomes in ostial PCI.
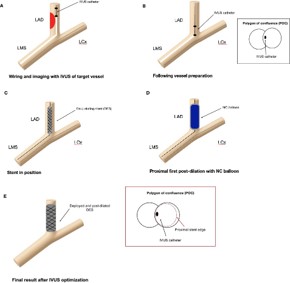
Proposed steps for FIX-IT
The FIX-IT technique involves a structured, image-guided approach to precise ostial stent placement (Figure 1). The procedure begins with standard wiring and IVUS imaging of the target lesion, followed by appropriate vessel preparation to optimize stent expansion. The IVUS catheter is then positioned at the vessel ostium, where the true anatomical origin is identified using both angiography and the Polygon of Confluence (POC) on IVUS. Cine angiograms are acquired with and without contrast while the IVUS remains in place, creating reference images that mark the exact ostial location.
After removing the IVUS catheter, the stent is carefully positioned so that its proximal edge aligns precisely with the previously identified IVUS marker. Understanding the relationship between the stent’s proximal struts and the balloon marker of the chosen platform is critical at this step. Cine angiography is repeated to confirm that the stent’s proximal edge corresponds exactly to the IVUS reference point before deployment.
The stent is then deployed at a pressure based on the distal reference vessel diameter. To minimize the risk of elongation or migration, proximal post-dilation is performed first [4], followed by Non-Compliant (NC) balloon optimization to ensure full expansion and apposition. The procedure concludes with a final IVUS run confirming optimal stent expansion and complete lesion coverage.
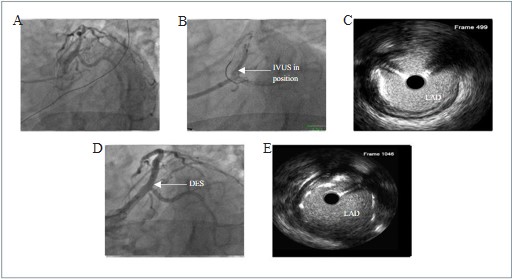
A 62-year-old gentleman underwent staged PCI to the Left Anterior Descending (LAD) artery following a prior intervention to the Right Coronary Artery (RCA). Angiography demonstrated moderate proximal and severe mid-LAD disease (Figure 2, Panel A). To avoid left main crossover stenting, IVUS assessment identified a suitable ostial LAD landing zone with a plaque burden of <40%. After adequate lesion preparation, an OptiCross Avvigo+ IVUS catheter (Boston Scientific, USA) was positioned angiographically at the LAD ostium (Figure 2, Panel B). IVUS imaging confirmed the radio-opaque marker to be at the POC (Figure 2, Panel C). A Xience Sierra 3.5×23 mm DES (Abbott Vascular, USA) was then deployed at nominal pressure, followed by proximal first post-dilation with a 4.5 mm NC balloon. The final angiogram demonstrated a well-expanded stent with no compromise of the Left Circumflex artery (LCx) (Figure 2, Panel D), and final IVUS confirmed precise ostial landing without protrusion into the left main coronary artery (LMCA) (Figure 2, Panel E).
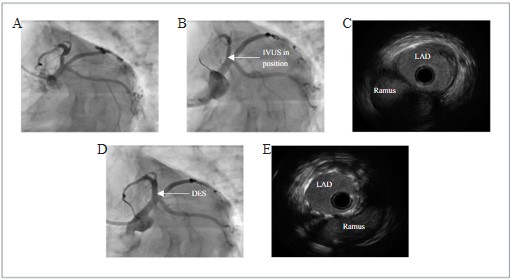
A 55-year-old female underwent coronary angiography after admission for Non-ST-Elevation Myocardial Infarction (NSTEMI). This demonstrated a severe proximal LAD stenosis (Figure 3, Panel A). IVUS confirmed extension of plaque burden >50% to the ostium, with minimal LMCA plaque. To avoid left main crossover stenting and potential jailing of the large calibre Ramus Intermedius (RI) and LCx arteries, the operator decided to stent the LAD to its ostium. A Truevision (Insight Lifetech, Shenzhen, China) IVUS catheter was positioned angiographically at the ostium of the LAD (Figure 3, Panel B). IVUS imaging confirmed that the radio-opaque marker of the catheter was seated just distal to the POC (Figure 3, Panel C). A Xience Skypoint 3.5×18 mm DES (Abbott Vascular, USA) was then successfully deployed using the IVUS marking cine as a guide, at nominal pressure. This was post-dilated from proximal to distal using a 3.5 mm NC balloon. A final angiogram showed a well deployed stent, with no pinching of the RI or LCx branches (Figure 3, Panel D). IVUS confirmed true ostial landing of the proximal stents, with no protrusion into the LMCA (Figure 3, Panel E).
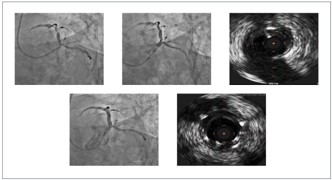
A 60-year-old gentleman, admitted for NSTEMI, underwent coronary angiography which revealed severe eccentric disease in the proximal-mid LAD (Figure 4, Panel A). After IVUS interrogation with a Volcano Eagle Eye IVUS catheter (Phillips, Netherlands), the lesion was prepared with scoring balloons. The operator decided to place the proximal edge of the stent at the LAD ostium to avoid left main crossover stenting and potential compromise of the sizeable LCx vessel. The IVUS catheter was then used to mark the LAD ostium angiographically (Figure 4, Panel B). Live IVUS imaging confirmed the position of the image transducer at the LAD ostium (Figure 4, Panel C). A Synergy Megatron 3.5x32 mm DES (Boston Scientific, United States) was then placed at the LAD ostium as guided by prior pictures, before being deployed at nominal pressure. Proximal first postdilation was performed with a 4.0 mm NC balloon, and more distally with a 3.5 mm NC balloon to varying pressures. Final angiogram showed a well deployed stent with no compromise of the LCx (Figure 4, Panel D). Final IVUS pullback confirmed accurate placement of the proximal stent edge at the LAD ostium with no protrusion into the LMCA (Figure 4, Panel E).
Technical considerations
Successful implementation of the FIX-IT technique requires attention to several key technical aspects to ensure accuracy and reproducibility across different anatomical scenarios and imaging systems.
Optimal angiographic projection
While the choice of angiographic projection remains important, it is not critical when using the FIX-IT technique. A major advantage of FIX-IT is its effectiveness even in patients with complex or overlapping anatomy, where conventional angiography may be limited. By using the IVUS catheter marker as the key reference for stent positioning, the need for multiple angiographic views—and thus both contrast use and radiation exposure—can be reduced.
When angiography is used alone, the selected projection should clearly visualize the vessel ostium with minimal overlap from adjacent structures such as the aortic cusps or neighboring branches. Orthogonal or slightly cranial/caudal angles may minimize foreshortening and improve ostial localization, with minor table or C-arm adjustments maintaining consistency.
However, angiography alone often fails to define the true ostium, even under optimal conditions. IVUS integration over comes this limitation by providing precise anatomical guidance, while angiography remains essential for final verification before stent deployment to ensure accurate positioning despite respiratory motion or patient movement.
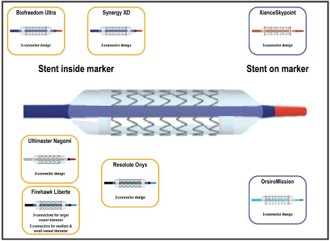
Choice of stent platform
Selecting an appropriate stent platform is critical for procedural precision. Operators should use a stent system they are familiar with, as the spatial relationship between the radioopaque marker and proximal stent struts varies across platforms (Figure 5). Understanding this marker-to-strut distance is essential for accurate alignment with the IVUS-defined ostium. Familiarity with these platform-specific characteristics enables precise ostial landing. This understanding of stent-specific marker positioning underpins the reproducibility and accuracy of the FIX-IT technique.
Relationship between IVUS imaging lens, radio-opaque markers and distal tip
Successful application of the FIX-IT technique requires precise understanding of the spatial relationship between the IVUS imaging lens, distal radiopaque marker, and catheter tip. Accurate awareness of this alignment enables proper matching of the IVUS imaging plane to angiographic landmarks, particularly the coronary ostium, during stent placement. The IVUS lens typically lies at or adjacent (proximal or distal) to the radioopaque marker, though this offset varies by catheter design and manufacturer. Unrecognized differences can cause geographic miss or aortic protrusion. (Table 1) summarizes these variations, which must be considered when performing angiographic–IVUS co-registration or fluoroscopic “X-mark” alignment.
| Brand | Distance from tip to distal marker | Distance from tip to imaging lens |
|---|---|---|
| Boston Opticross | 5 mm | 20 mm |
| Terumo Anteowl | N/a | 8 mm |
| Terumo Altaview | N/a | 22 mm |
| Nipro Makoto Dualpro | 5 mm | 16 mm |
| Insight Lifetech | 5 mm | 20 mm |
| Philips Refinity | N/a | 20.5 mm |
| Philips Eagle Eye Platinum | N/a | 10 mm |
| Philips Eagle Eye Platinum ST | N/a | 2.5 mm |
Minimizing guide and patient movement
Maintaining guide catheter stability is critical during both IVUS marking and stent deployment. Even subtle guide movement, often caused by deep inspiration, expiration, or patient motion, can lead to small but clinically significant geographic miss. Operators should carefully observe for any catheter drift during the initial IVUS marking and aim to preserve a consistent respiratory pattern throughout deployment. Practical measures include employing guide stabilization techniques, such as the use of a buddy wire or floating aortic wire, to minimize unintended movement and maintain precise alignment between the IVUS-defined and fluoroscopic reference points.
The FIX-IT technique is a practical, image-guided approach for ostial PCI that aligns IVUS anatomy with real-time fluoroscopy to achieve precise, reproducible stent placement at the true vessel origin. Applicable across IVUS platforms and diverse cases, it integrates easily into routine practice. FIX-IT facilitates accurate ostial stent landing and optimization without requiring proprietary software or specialized tools beyond standard IVUS and fluoroscopy, ensuring broad accessibility. As PCI advances toward precision-guided therapy, FIX-IT offers a valuable option for complex anatomy. While further studies are needed to assess long-term outcomes, our experience supports its effectiveness in enhancing technical success and operator confidence in ostial interventions.
Take home messages
• FIX-IT enables precise fluoroscopic localization of the anatomical coronary ostium by directly translating IVUSderived landmarks into real-time procedural guidance.
• By addressing angiographic limitations such as foreshortening and anatomic overlap, the technique reduces ostial geographic miss and optimizes stent landing accuracy.
• Its reproducibility across multiple IVUS platforms supports FIX-IT as a robust, imaging-integrated strategy to improve technical and clinical outcomes in ostial PCI.
