-
Email [email protected]
-
Address 848 N. Rainbow Blvd. #5486 Las Vegas, NV 89107, USA
1Department of Anaesthesiology and Intensive Care, University Hospital of Southern Denmark & Department of Regional Health Research, University of Southern Denmark.
2Heart, Lung and Vessel, Aarhus University Hospital, Denmark.
*Corresponding author: Carl-Johan Jakobsen
Department of Anaesthesiology, Aarhus University Hospital, 8200 Aarhus N, Denmark.
Email ID: [email protected]
Received: Dec 23, 2025
Accepted: Jan 21, 2026
Published Online: Jan 28, 2026
Journal: Annals of Cardiology
Copyright: Jakobsen C et al. © All rights are reserved
Citation: Bhavsar R, Jakobsen C. Female health inequalities in handling cardiovascular disease. Ann Cardiol. 2026; 3(1): 1016.
Introduction: Despite reductions in the incidence and mortality of Cardiovascular Disease (CVD) in the last decades it still accounts over 30% of worldwide deaths. Although females experience higher mortality the current clinical IHD guidelines do not distinguish between sexes and despite added diagnostic procedures the differences remain. This study aimed to describe and evaluate effect, outcomes and health inequalities associated with the increased number of diagnostic procedures. Methods: The study included 280,296 first-entry patients registered in the mandatory Western Denmark Heart Registry from 2000-2020. Mortality was evaluated with Kaplan-Meier curves and further compared to background population to attenuate the long study period. Results: Females constituted 39.7% of all first-entry diagnostic procedures but only 25.5% of patients undergoing invasive cardiac treatments, demonstrating a possible female underestimation with substantially lower treatment rate compared to males. Further, the number of procedures per patient was diverging as well, being 2.53 in males vs. 1.84 in females in 2020. Female 10-year mortality were higher in treatment groups 1.28(1.24-1.31) but lower in the non-treated patients 0.71(0.670.73). Compared with the background population the non-treated patients revealed substantially lower mortality. The comparison with background mortality further indicated a difference in patients characteristics in referral to CTA or ICA showing great differences between mortality after CTA compared to ICA in especially non-treated patients. Conclusion: Females seem referred to diagnostic procedures in accordance with prevalence of cardiac disease but obtain substantially lower number of invasive cardiac treatment procedures, both in absolute number and number per person, compared to males. Further females present substantially higher mortality after PCI and cardiac surgery as well. In contrary, females only facing diagnostication showed significantly better survival than males, both studies related and compared to the background population.
Keywords: Cardiovascular diseases; Coronary artery disease; Healthcare disparities; Health inequalities ischemic heart disease; Sex differences; Invasive cardiac procedures.
Despite the huge reductions in the incidence and mortality of Cardiovascular Disease (CVD) particularly in developed countries [1,2], CVD still accounts for over 30% of worldwide death, with Ischaemic Heart Disease (IHD) being the leading cause, accounting for 16% in 2019 [1-3]. Contributors to the positive development are likely lifestyle changes, enhanced surveillance and diagnostic practices together with improved medical therapy and augmented coronary revascularization [4,5].
Despite uniform efforts and contrary to expectations females still experience higher IHD related mortality than males [6-8]. Factors governing this disproportion are believed to include older age at referral, more frequent presentation with atypical symptoms, and less frequent use of evidence-based therapies among females [8-10]. Additionally females experience poorer prognosis after acute cardiovascular events indicating a higher cardiovascular risk profile [11]. This risk may be underestimated perhaps due to the perception that women protected against CVD, resulting in lower rates of diagnostic angiograms and interventional procedures as compared to men [5,12-14].
Diagnostic algorithms for suspected chronic coronary syndrome have changed considerably with the introduction of computed tomography angiography (CTA) as a first-line modality around 2007–2008, aiming to reduce invasive coronary angiography (ICA) unlikely to result in revascularization. However, data from the Western Denmark Heart Registry (WDHR) demonstrate a marked increase in CTA without a corresponding increase in invasive treatments, suggesting expanded indications beyond the original gatekeeping role.
Using WDHR data from 2000 to 2020, this study aimed to describe diagnostic trends, clinical outcomes and sex related differences associated with the large proportion of diagnostic procedures.
The data were obtained from WDHR comprising information of all cardiac diagnostic and interventional procedures performed in adult patients from the Western Denmark. Reporting to WDHR is mandatory and initially included Intervascular Coronary Angiography (ICA), Percutaneous Coronary Intervention (PCI) and cardiac surgery. CTA and Transcatheter Aortic Valve Replacement (TAVR) was added in 2008.
Data are registered prospectively, including detailed patient-, risk-, procedure-, and care-related data and are integrated in to into dally clinical practice [18]. WDHR is known for its high accuracy and completeness ensured through systematic validation procedures [19]. All data related to this study have been obligatory since 2006. Earlier data fields were considered zero or negative, if no corresponding data were registered in the relevant variables.
All Danish citizens have a unique Civil Personal Registration (CPR) number assigned at birth or immigration and kept throughout life, enabling cross-linking between different health and civil registries, ensuring feasibility to conduct large, population-based studies with relevant outcome follow-up on all procedures and treatments [13,14,20].
Data handling was approved and registered by the Danish Data Protection Agency (1-16-02-455-21). Written consent is not required for registry-based studies according to Danish legislation. The handling and use of data followed the agency’s directions were fully met.
Study population
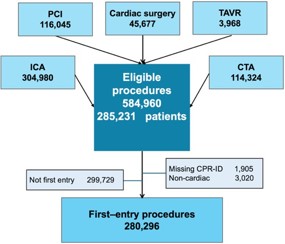
All WDHR registrations between 2000 and 2020 were considered for eligibility (Figure 1). Patients without valid CPR and referrals for non-cardiac indication was excluded from detailed analysis. Additional was all later procedures after the index procedure if undergoing multiple procedures to isolate and create a cohort of first-entry procedures.
Procedure indications were grouped into major indications: ACS, CCS, valvular heart disease, arrhythmias, cardiac insufficiency/cardiomyopathy, cardiogenic shock/cardiac arrest) and other. If overlapping indications, the case was allocated the most severe indication, i.e. CABG and valve allocated to the valve group.
Some history derived factors in WDHR, including the recorded indication, are inherited from the previous registration independent of procedure type or treatment. Consequently, the inherited indications may be inaccurate and in doubt changed, based on registered ICD-10 code in registered referral formular (Supplement 1).
Outcome parameters
The main analysis was association between diagnostication procedures and following invasive treatment procedures i.e. PCI, cardiac surgery and TAVR with primary focus on changes over time and sex differences. The primary outcome was all cause mortality / survival after stipulated periods over the 20year study period.
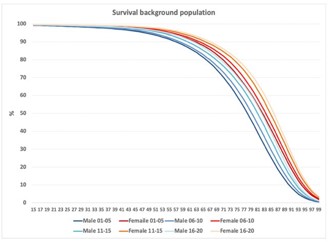
Considering sex differences in life expectancy combined with relatively large change in mean living time over the 20-years study period, all patients were assigned an estimated 1and 5-year risk of death based on actual 5-years life tables (Supplement 1,) acquired from Denmark Statistics [21]). These expected 1and 5-year mortality risk were based on year of procedure, age, and sex, enabling analyses of the study’s actual mortality against the background population mortality in a 1:1 ratio.
Statistical analyses
| No | % | Per person | Fraction | ||
|---|---|---|---|---|---|
| Invasive coronary angiography | Male | 132.581 | 64,3% | 1,534 | 77,1% |
| Female | 73.537 | 35,7% | 1,382 | 64,9% | |
| p-value | <0.0001 | <0.0001 | |||
| Computed coronary angiography | Male | 52.379 | 51,1% | 1,126 | 30,5% |
| Female | 50.081 | 48,9% | 1,105 | 44,2% | |
| p-value | <0.0001 | <0.0001 | |||
| Percutaneous coronary intervention | Male | 63.269 | 72,7% | 1,354 | 36,8% |
| Female | 23.802 | 27,3% | 1,276 | 21,0% | |
| p-value | <0.0001 | <0.0001 | |||
| Cardiac Surgery | Male | 32.867 | 74,1% | 1,028 | 19,1% |
| Female | 11.501 | 25,9% | 1,033 | 10,2% | |
| p-value | 0.030 | <0.0001 | |||
| Transthoracic aortic replacement | Male | 2.205 | 55,9% | 1,005 | 1,3% |
| Female | 1.740 | 44,1% | 1,007 | 1,5% | |
| p-value | 0.281 | <0.0001 | |||
| All | Male | 172.006 | 60,3% | 2,232 | |
| Female | 113.225 | 39,7% | 1,775 | ||
| p-value | <0.0001 |
Patients were divided by age, sex, indication and procedure types for the detailed statistical analyses. Categorical variables were analysed using the χ2-test, and continuous variables by Students independent t-test and ANOVA. Kaplan‒Meier survival curves were used to evaluate outcomes over time. Analyses were performed with MedCalc® software version 23.4 (Mariakerke, Belgium). A probability value of <0.05 was used to define statistical significance.
The selection process revealed 584,994 registered procedures in 285,231 patients. The primary exclusions were 1,905 without valid ID (CPR) and 3020 non-cardiac indications, together with 299,729 not first-entry cases, isolating a cohort of 280,296 first-entry procedures analysis (Figure 1).
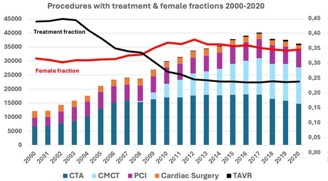
During the two decades the number of procedures increased constantly from 2000 to 2017 after which was seen a minor fall in ICA, PCI and cardiac surgery while marginal increases in TAVR and CTA was seen in this period (Figure 2). The overall result was a decline in invasive treatments falling from 45.5% in 2002 to 23.4 % in 2020. Concerning first entry procedures numbers increased from 7,133 in 2001 to 17,623 in 2017 ending on 15,822 in 2020. Overall, an almost 2.5-fold increase in diagnostic procedures compared to only a 56% increase of invasive treatments.
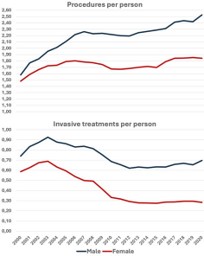
Females accounted for 34.1% of all entries, with a small increase from 30.1% in 2002 to 35.8% in 2014 (Figure 2). Males was submitted to substantially more procedures per person than females with a small difference in 2000, 1.58 vs. 1.48, increased to 2020 to 2.53 vs. 1.84 (Figure 3), but with great variations highest in ICA and PCI (Table 1) and further revealed lower fractions in all procedure types with highest 48.9% in CTA to lowest 25.9% in cardiac surgery (Table 1; P<0.0001; χ2-test). In the same period the invasive treatments per person declined from 0.74 and 0.59 respectively in 2000 to 0.70 and 0.28 (Figure 3).
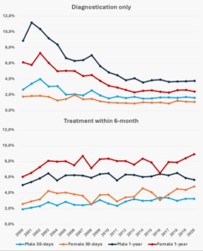
Analysing only on the first-entry procedures the female fraction was a little higher 39.7%, but lower fraction in all procedure types, except in diagnostication only where more females was submitted to CTA compared to men (Table 1). Diagnostication only was more frequent in females compared to males, 69.2% vs. 47.2% respectively.
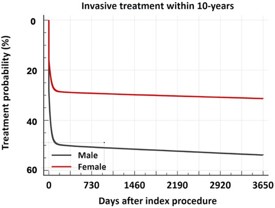
Underlining the differences was also the fraction of invasive treatment, showing that females was substantially less treated especially within first week after diagnostication procedures being 31.2% vs. 17.4% on day 4 and 41.0 vs. 22.5 on day 30 after diagnostication (Figure 4).
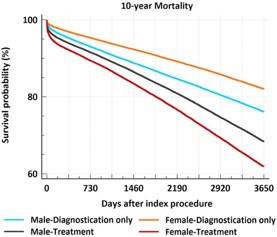
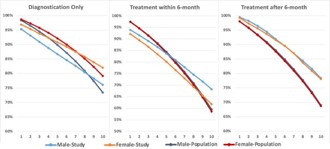
In the early period the short time mortality was higher in patients not submitted to evasive treatment after ICA/CTA than patient submitted to PCI, cardiac surgery or TAVR within 6-month (Figure 5). Overall treated females had higher mortality than males (30-days 3.69% vs. 2.78% and 1-year 7.78% vs. 6.04%) while in non-treated female mortality was lower (30days 1.29 vs. 2.11 and 1-year 3.87 vs. 5.87). This is enhanced in 10-year mortality indicating rather great differences both related to treatment within 6-month and sex (Figure 6), with higher female mortality in treated patients 1.28(1.24-1.31). In contrast the female mortality was lower in non-treated groups 0.71(0.69-0.73). Comparing to the background population demonstrated that male did better than the background earlier than females in treated group, while females did better in diagnostication only (Figure 7).
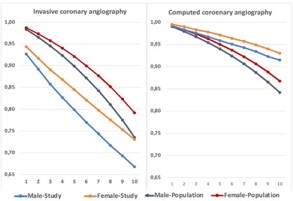
Concerning the group diagnostication only, great differences was found in survival when comparing sex and the background population (Figure 8). Female had better survival in both ICA 0.71 (0.69-0.73) and CTA 0.76 (0.71-0.81). Compared to background population the differences were huge as ICA patients never reached the background population while the CTA patients from start had a better survival than the background population.
We analysed periprocedural data from 584,960 cardiac procedures comprising 280,296 first-entry patients undergoing CVD diagnostic procedures between 2000 and 2020. The main emphasis was on differences in the management and outcome between patients undergoing an invasive procedure with in the first 6-month and those managed with diagnostic evaluation only by Invasive Coronary Angiography (ICA) or Computed Tomography Angiography (CTA), with a primary focus on sex differences. Female referral more often ended after diagnostic procedure being 69.5% compared to 47.2% in males. In agreement with earlier publications, females demonstrated higher mortality in both early and late invasive treatment [8,21,22], but in contrary notably a higher survival than males in the nontreated patients.
The absolute number of invasive treatments increased from 3,569 peaking in 2017 with 8,916 procedures. However, due to a far greater escalation, especially following implementation of CTA in 2007/2008, the fraction of invasive treatment gradually declined over the decades, from 45.5% in 2002 to 23.3% in 2019. An additional contributing factor was an increase in the number of procedures per person, rising from 1.55 to 2.24 overall. This increase was more pronounced in males (from 1.56 to 2.53) than in females (from 1.48 to 1.84) (Figure 3).
Differences in procedures per person were observed for ICA, CTA and PCI, whereas no difference was seen for TAVR and only a marginally higher rate was observed in cardiac surgery. The latter finding is somewhat unexpected, as the overall female fraction undergoing surgery, is approximately close to half of males, (10.2% vs. 19.1%, Table 1), a pattern that nevertheless aligns with previous studies focusing on specific cardiac surgical procedures [13,14,22].
In Denmark, females account for 39% and males for 61% of IHD patients [21,23], closely matching the 39.7% and 60.3% representation among the 280,296 first-time entries in this study from WDHR. As females only accounted for 34.1% of all WDHR registrations, reflecting the impact of differences in the number of procedures per person. Only 30.8% of females compared with 52.8% of males were submitted to invasive treatment procedures; consequently, females accounted for 25.5% and males for 74.5% of all invasive treatments—a disparity that is not readily explained.
In recent years, females have contributed 43.9% of consultations in primary care, marginally exceeding their IHD prevalence, suggesting equitable conservative referral practices in the primary sector. Consequently, the underrepresentation of females appears to arise within hospital care after diagnostic evaluation. The lower invasive treatment activity in females may partly originates from comparatively more healthy females being referred for diagnostic procedures, evaluated by the fact that non-treated females showing better survival than both men and female background population, especially after CTA (Figure 8).
In contrast to patients diagnosed by Invasive Coronary Angiography (ICA), patients evaluated by Computed Tomography Angiography (CTA) demonstrated markedly better survival than the background population in both sexes. This survival difference between the ICA and CTA-diagnosed patient groups agrees with earlier studies in patients with chronic coronary syndrome, suggesting that a substantial proportion of patients without evident or treatable coronary disease are referred for CTA evaluation [24].
There has been concern that the rapidly increasing use of CTA might lead to higher numbers of ICA or even Percutaneous Coronary Intervention (PCI) procedures due to false-positive CTA findings [25-27]. However, this does not appear to be the case, as the number of ICA procedures has gradually declined over the past decade, despite an overall increase in invasive treatment activity.
Divergent to invasive treatment groups, non-treated females showed better survival than males (Figure 6). Regarding the mortality in invasive treatment both 30-days and 1 year has increased marginally during the period, especially due to increased number of ACS and TAVR in higher age patients. In contrast the mortality has decreased substantially likely due to the increased number of diagnostication not resulting in invasive treatment. The findings are supplemented by comparisons with the background population, demonstrating that invasive treated patients present hirst of all higher mortality than nontreated, but also do relatively worse compared to background population (Figure 7).
Despite a greater decline, even higher than males, in CVD-related mortality during the last decades, females still encounter a higher mortality [6-8]. This disparity is believed to be caused by factors such as older age, more comorbidities and risk factors, a greater incidence of procedural complications, and less frequent use of evidence-based invasive therapy [8,9,28,29].
Strengths and limitations
A key advantage of this study is its large, representative cohort from the WDHR with almost 585,000 registered entries of which 280. 296 first-entry patients was obtained. The number augments the analysing and trustworthiness of the findings. The essential strengths are the mandatory and obligatory nature of the data which predominately are registered and reported prospectively from a well-defined uptake area into a shared mandatory database used by all relevant institutions. The large cohort with detailed in-hospital outcome and complete mortality follow-up on all patients undergoing invasive cardiologic and cardiac surgery procedures for more than 2 decades allows robust estimations of patients, results, and adverse events.
Nonetheless, the study caries inherent limitations and especially the non-randomized nature may cover additional effects of missing covariates and potentially increase confounding. Further, the observational bearing might introduce biases and muddling factors. Although, the public free health care system with uniform structure and treatment practices reduce variability, but the long study period poses challenges from possible changes in clinical procedures. Finally, the large number makes even small differences statistically significant enhancing that data shown an association and not cause or reason for conclusions.
Despite referred to diagnostic cardiac procedures, in accordance with the prevalence of cardiovascular disease, they obtain substantially lower number of cardiac diagnostication and treatment procedures, both in absolute number and number per person compared to males. Despite improvement in recent decades the still presents a substantially higher mortality after PCI and cardiac surgery as well. In contrary, females only facing diagnostication showed significantly better survival than males, both study related and compared to the background population.
Abbreviations: ACS: Acute coronary syndrome; CABG: Coronary arterial bypass grafting; CCS: Chronic coronary syndrome; CTA: Computed Tomography Angiography; CPR: Civil Personal Registration; CVD: Cardiovascular Disease; ICA: Invasive Coronary Angiography; ICD-10: International Classification of Diseases, 10th revision; IHD: Ischaemic Heart Disease; PCI: Percutaneous Coronary Intervention; TAVR: Transcatheter Aortic Valve Replacement; WDHR: Western Denmark Heart Registry.
Ethics approval and consent to participate: Database study registered by the Danish Data Protection Agency (1-16-02-45521). According to Danish legislation, consent is not required for registry-based studies.
Funding: Except support from authors clinics, no external funding.
Disclosures: The authors have nothing to disclose.
Availability of data and materials: The datasets generated for use in the current study are not publicly available as part of the Danish patient/hospital system, but limited blinded data are available from the corresponding author on reasonable request and subsequent permissions from hospital/database managers.
Competing interests: The authors have no competing interest.
Disclosures: The authors have nothing to disclose.
Authors’ contributions: CJJ and RB study design; CJJ data acquisition and analysis; RB and CJJ writing, re-writing and critical review.
