-
Email [email protected]
-
Address 848 N. Rainbow Blvd. #5486 Las Vegas, NV 89107, USA
1Pontifícia Universidade Católica de São Paulo, Sorocaba, Brazil.
2Universidade Federal do Ceará, Fortaleza, Brazil.
3Universidade Federal da Paraíba, João Pessoa, Brazil.
4Universidade Federal Fluminense, Niterói, Brazil.
5Hospital Sírio-Libanês, São Paulo, Brazil.
6Hospital Municipal de Badalona, Barcelona, Spain.
7Universidad Católica Argentina, Buenos Aires, Argentina and Duke University, Durham, North Caroline, United States.
*Corresponding author: Juliana Martins Giorgi
Heart Failure Specialist Medical Doctor, Institution: Sírio Libanês Hospital, Dr Melo Alves, N 89 #422, Jardim América, ZIPCODE: 1417010, São Paulo, São Paulo, Brazil.
Tel:+ 5511 981216101; Email ID: [email protected]
Received: Jan 20, 2026
Accepted: Feb 27, 2026
Published Online: Mar 06, 2026
Journal: Annals of Cardiology
Copyright: Giorgi JM et al. © All rights are reserved
Citation: Seixas MM, dos Santos Silva RRA, Batista PG, da Conceição LD, Giorgi JM, et al. Selective aldosterone synthase inhibitors for resistant or uncontrolled hypertension: An updated systematic review and meta-analysis of randomized controlled trials. Ann Cardiol. 2026; 3(1): 1017.
Illustration of the effects of selective Aldosterone Synthase Inhibitors (ASIs) in patients with resistant or uncontrolled Hypertension (HTN). ASIs significantly reduce systolic blood pressure (SBP, Mean Difference [MD] –8.44 mmHg; 95% Confidence Interval [CI] –10.13 to –6.76; p<0.0001), but increase the risk of hyperkalemia, hyponatremia, and hypotension. The meta-analysis included five Randomized Controlled Trials (RCTs) with 2,637 patients (mean age 61.2 years, 56% male, 36% with Type 2 Diabetes Mellitus [T2DM]), and follow-up ranging from 8 to 52 weeks (w). Risk Ratio (RR) and p-values are shown for safety events.
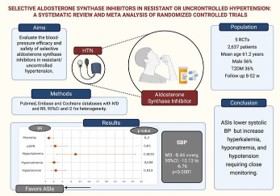
Background: Resistant and uncontrolled hypertension remains challenging to clinically manage. This meta-analysis of phase II/III Randomized Controlled Trials (RCTs) evaluated the efficacy and safety of selective Aldosterone Synthase Inhibitors (ASIs) for blood pressure control.
Methods: MEDLINE, Embase, and Cochrane (to Aug 2025) were searched for RCTs of selective ASIs vs placebo in resistant/ uncontrolled hypertension [1]. Our main endpoint was change in systolic blood pressure; additional endpoints included electrolyte disorders [2], hypotension, and renal effects. We pooled outcomes in a random-effects meta-analysis using Mean Difference (MD) for continuous and Risk Ratio (RR) for binary endpoints, along with 95% Confidence Intervals (CIs). A p-value<0.05 was considered statistically significant.
Results: Five RCTs involving 2,637 patients were included. Selective ASIs significantly reduced systolic blood pressure (MD–8.44 mmHg; 95% CI –10.13 to –6.76; P<0.0001) when compared to placebo. Risks of hyperkalemia (RR, 9.45 [95% CI, 2.99 to 29.87]; P=0.0001), hyponatremia (RR, 2.12 [95% CI, 1.27 to 3.56]; P=0.0042), and hypotension (RR, 2.72 [95% CI, 1.23 to 6.00]; P=0.0135) were higher with ASIs. No significant differences between groups were observed for mortality (RR, 0.30 [95% CI, 0.05 to 1.93]; P=0.2063) or estimated glomerular filtration rate decline (RR, 2.50 [95% CI, 0.97 to 6.46]; P=0.0584).
Conclusion: Selective ASIs lower systolic blood pressure in resistant/uncontrolled hypertension, but risks of hyperkalemia, hyponatremia, and hypotension limit use and require monitoring. Longer trials should confirm cardiovascular/renal benefit and clarify long-term safety.
Keywords: Resistant hypertension; Selective aldosterone synthase inhibitors; Systolic blood pressure.
Abbreviations: AE: Adverse event; ASI(s) – Aldosterone synthase inhibitor(s); BMI: Body mass index; BP: Blood pressure; CI(s): Confidence interval(s); CKD: Chronic kidney disease; eGFR: Estimated Glomerular Filtration Rate HT; HTN: Hypertension; MD: Mean difference; MRA(s): Mineralocorticoid receptor antagonist(s); PRISMA: Preferred reporting items for systematic reviews and meta-analyses; PROSPERO: International prospective register of systematic reviews in health and social care; RAAS: Renin–angiotensin–aldosterone system; RCT(s): Randomized controlled trial(s); RoB 2: Risk of bias 2; RR: Risk ratio; SAE: Serious adverse event; SBP: Systolic blood pressure; SD(s): Standard deviation(s); SGLT2: Sodium glucose cotransporter; T2DM: Type 2 diabetes mellitus.
Hypertension remains one of the most significant global contributors to cardiovascular morbidity and mortality, affecting over one billion adults worldwide. Among treated individuals, a substantial proportion continue to exhibit uncontrolled or resistant hypertension despite adherence to multidrug therapy [1]. This population carries a markedly elevated risk of adverse cardiovascular outcomes, highlighting an urgent need for therapeutic innovations beyond conventional Renin–Angiotensin–Al-dosterone System (RAAS) blockade [1,2]. Across international cohorts, dysregulated aldosterone synthesis has emerged as a central driver of treatment resistance, promoting sodium retention, vascular inflammation, myocardial and renal fibrosis, and impaired natriuresis [3]. While mineralocorticoid receptor antagonists provide essential benefits, their use is limited by hyperkalemia and endocrine adverse effects, especially in patients with chronic kidney disease or diabetes. These limitations have generated renewed interest in upstream strategies that target aldosterone production itself [4].
Selective Aldosterone Synthase Inhibitors (ASIs) directly inhibit CYP11B2, the terminal enzyme responsible for aldosterone biosynthesis. First generation ASIs demonstrated antihypertensive potential but lacked sufficient selectivity, leading to cortisol suppression [5]. Recent advances in medicinal chemistry led to second-generation agents, such as lorundrostat, baxdrostat, and BI 690517, with marked improvements in CYP11B2 specificity and favorable early safety signals [57]. Phase II and III clinical trials have shown consistent reductions in systolic blood pressure among patients with resistant or uncontrolled hypertension [5,811]. However, prior systematic reviews did not fully capture the maturing evidence base. Earlier analyses combined first and second-generation ASIs, included heterogeneous hypertensive populations, and were limited by the absence of contemporary phase III data. Consequently, the international relevance and clinical applicability of prior pooled estimates remained uncertain [12].
This updated systematic review and meta-analysis were therefore conducted to address these gaps by synthesizing evidence exclusively from selective second-generation ASIs, focusing solely on patients with resistant or uncontrolled hypertension, and incorporating all available phase II and III trials through 2025. This approach provides the most precise and clinically relevant evaluation of their efficacy and safety to date.
This systematic review and meta-analysis were prospectively registered in the International Prospective Register of Systematic Reviews in Health and Social Care (PROSPERO; CRD420251130080) and conducted in accordance with the Cochrane Collaboration Handbook for Systematic Reviews of Interventions [13] and the Preferred Reporting Items for Systematic Reviews and Met-analyses (PRISMA) Statement guidelines [14]. Our study did not require informed consent or an Institutional Review Board approval, as we incorporated secondary deidentified data from publicly available studies.
To enhance reproducibility and address intertrial heterogeneity, we extracted and summarized each study’s operational definitions of resistant versus uncontrolled hypertension, background antihypertensive therapy requirements, and blood pressure entry thresholds, which are detailed in Table 2.
Study eligibility
We included phase 2 or 3 RCTs that enrolled adults (≥18 years) with uncontrolled or resistant hypertension, as defined by individual study protocols. We compared a selective aldosterone synthase inhibitor (ASI) with a placebo on the background of standard antihypertensive therapy. We excluded phase 1 studies, observational designs, case reports, case series, and trials involving broader or mixed hypertensive populations not explicitly limited to resistant or uncontrolled hypertension.
Key differences in eligibility criteria, background therapy, and systolic blood pressure thresholds across trials are summarized in Table 2.
When overlapping populations were identified, the dataset with the most complete and recent outcome data was retained to avoid duplication. Trials that did not report extractable quantitative data for at least one predefined endpoint were also excluded.
Search strategy and data extraction
We systematically searched MEDLINE (PubMed), Embase, Cochrane Central Register of Controlled Trials (CENTRAL) from inception through September 2, 2025, without language restrictions. Search terms included: “hypertension”, “high blood pressure”, “high blood pressures”, “elevated blood pressure”, “aldosterone dysregulation”, “blood pressure elevation”, “resistant hypertension”, “chronic kidney disease”, “uncontrolled hypertension”, “lorundrostat”, “MT4129”, “baxdrostat”, “CIN107”, “aldosterone synthase inhibitor”, “CYP11B2 inhibitor”, “BI 690517” “BI 689648”. Reference lists of included studies and prior systematic reviews were screened manually (backward snowballing) to identify additional eligible reports.
All references were imported into Zotero for deduplication and blinded title–abstract screening. Two independent reviewers (M.M.S. and R.R.A.S.S.) assessed each citation for eligibility, and disagreements were resolved by consensus or third-reviewer adjudication. Full-text articles meeting inclusion criteria were extracted using a standardized form, and extracted data were cross-verified by an independent investigator to ensure accuracy.
Endpoints and subgroup analysis
Primary efficacy endpoints included the change in Systolic Blood Pressure (SBP) from baseline to the end of follow-up. Secondary outcomes were diastolic BP reduction, all-cause mortality, hypotension (symptomatic or requiring intervention), hyperkalemia, hyponatremia, hypercortisolism, hypocortisolism, Estimated Glomerular Filtration Rate (eGFR) decline, any Adverse Event (AE), and Serious Adverse Events (SAE). Subgroup analyses were performed for endpoints with at least one study available for each selective ASI, enabling cross-drug comparisons (baxdrostat, lorundrostat, BI 690517). When subgrouping was not feasible, the specific drug represented in each forest plot was explicitly indicated.
Definitions of eGFR decline varied across trials. BrigHTN and the NEJM baxdrostat trial defined decline as a categorical ≥30% reduction from baseline, whereas lorundrostat trials reported investigator-determined renal adverse events or absolute changes in eGFR. These definitions were abstracted individually and incorporated into the pooled analysis.
Risk of bias assessment
Risk of bias was evaluated using version 2 of the Cochrane Collaboration’s Risk of Bias Tool for randomized Trials (RoB 2) [15], which classifies studies as low, some concerns, or high risk of bias across five domains (selection, performance, detection, attrition, and reporting). Two independent reviewers (M.M.S. and R.R.A.S.S.) performed all assessments, with discrepancies resolved by consensus.
Sensitivity analysis
A leaveoneout sensitivity analysis was conducted for outcomes reported in at least three studies to assess the robustness of the results. This approach sequentially omits one survey at a time and recalculates pooled effect estimates for each iteration. Sensitivity analysis was prespecified for the primary endpoint of systolic BP reduction, the most consistently reported efficacy measure across trials.
A prespecified secondary sensitivity analysis excluded trials that enrolled patients with uncontrolled hypertension but did not strictly meet resistant-hypertension criteria. This analysis evaluated whether SBP reduction remained consistent when restricting the dataset to fully resistant populations.
Data analysis
For binary outcomes, pooled Risk Ratios (RRs) and 95% Confidence Intervals (CIs) were calculated; for continuous outcomes, Mean Differences (MDs) with 95% CIs were derived. When Standard Deviations (SDs) were not reported, they were imputed from standard errors, CIs, or interquartile ranges using formulas recommended in the Cochrane Handbook (Section 6.5.2.10) [16]. When multiple arms were combined, pooled SDs were calculated using the same standard methods.
Meta-analyses were conducted using a random-effects model (DerSimonian–Laird method) to account for clinical and methodological heterogeneity. Between-study heterogeneity was evaluated using the Cochrane Q test (p<0.10 considered significant) and quantified with the I² statistic (I²>25% indicating heterogeneity). Studies with zero events in both arms were excluded from pooled analyses, as per Cochrane recommendations (Section 10.4.4.2) [17]. Statistical significance was defined as a two-tailed p<0.05
All analyses were performed using R software (version 4.5.0; R Foundation for Statistical Computing) with the meta and meta for packages.
The search strategy identified 424 records (Figure 1). After removal of duplicates and screening of titles and abstracts, 20 studies were assessed in full according to predefined eligibility criteria. Ultimately, five randomized controlled trials [5,8–11] met all inclusion criteria, representing a nonoverlapping population of 2,637 patients. The main reasons for exclusion were nonselective ASI use (n=7), nonrandomized or open-label design (n=5), and mixed hypertensive populations not limited to resistant or uncontrolled hypertension (n=3). Baseline characteristics of the included population are summarized in Table 1. The mean age across studies was 61.2 years, and 56% of participants were men. The average Body Mass Index (BMI) was 32.1 kg/m², reflecting a predominantly obese population, while 944 participants (36%) had diabetes mellitus.
Pooled analyses of all studies
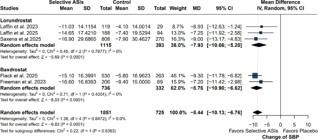
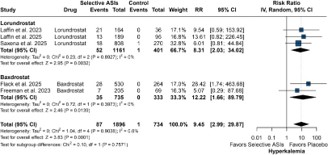
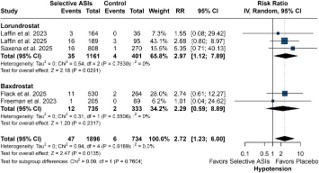
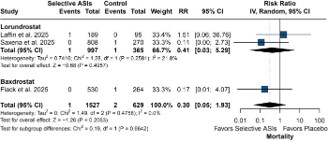
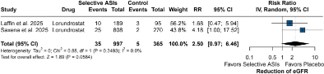
Across all included studies, ASIs were associated with a significant reduction in SBP compared with placebo (mean difference –8.44 mmHg; 95% Confidence Interval [CI] –10.13 to –6.76; p<0.0001; I²=0%; Figure 2). Regarding safety outcomes, the use of selective ASIs was associated with higher risks of hyperkalemia (Risk Ratio [RR] 9.45; 95% CI 2.99–29.87; p=0.0001; I² = 0%; Figure 3), hyponatremia (RR 2.12; 95% CI 1.27–3.56; p=0.0042; I²=0%; Figure 4), and hypotension (RR 2.72; 95% CI 1.23–6.00; p=0.0135; I²=0%; Figure 5). No significant differences between groups were observed for all-cause mortality (RR 0.30; 95% CI 0.05–1.93; p=0.2063; I²=0%; Figure 6) or for reduction in Estimated Glomerular Filtration Rate (eGFR) (RR 2.50; 95% CI 0.97–6.46; p=0.0584; I²=0%; Figure 7).
Absolute event rates were low but clinically relevant. Across included trials, hyperkalemia occurred in 1.6–9.8% of ASI treated participants versus 0–1.2% with placebo. Thresholds used to define hyperkalemia varied slightly: baxdrostat trials used serum potassium ≥5.5 mmol/L; lorundrostat trials used ≥5.5–6.0 mmol/L; and BI 690517 used ≥6.0 mmol/L or an increase judged clinically significant. Absolute hyperkalemia event rates, placebo comparisons, maximum dose risks, and trial specific potassium thresholds are detailed in Table 3.
Subgroup analyses
In subgroup analyses, both lorundrostat and baxdrostat significantly reduced SBP compared with placebo. The mean difference for lorundrostat was –7.93 mmHg (95% CI –10.66 to –5.20; p<0.0001; I²=0%), and for baxdrostat –8.76 mmHg (95% CI –10.90 to –6.62; p<0.0001; I²=0%), with no significant difference between drugs (Pinteraction=0.6363). These findings indicate that both agents achieved comparable antihypertensive efficacy with minimal between study heterogeneity. Regarding safety, lorundrostat was associated with increased risks of hyperkalemia (RR 8.31; 95% CI 2.03–34.02; p=0.0032), hyponatremia (RR 2.03; 95% CI 1.18–3.49; p=0.0106), and hypotension (RR 2.97; 95% CI 1.12–7.89; p=0.0291). Baxdrostat also demonstrated a higher incidence of hyperkalemia (RR 12.22; 95% CI 1.66–89.79; p=0.0139), although the results for hyponatremia (RR 3.35; 95% CI 0.61–18.30; p=0.1620) and hypotension (RR 2.29; 95% CI 0.59–8.89; p=0.2317) did not reach statistical significance. The between drug differences were not statistically significant for any of these safety outcomes (Pinteraction>0.05). Lo rundrostat showed no significant effect on mortality compared with placebo (RR 0.41; 95% CI 0.03–5.29; p=0.4957), and only one baxdrostat study reported mortality events, preventing a pooled subgroup meta-analysis for this agent (Figure 6).
Sensitivity analyses
Leave-one-out sensitivity analysis for the primary endpoint of SBP reduction demonstrated consistent results with the overall findings, confirming the robustness of the pooled estimates. No single study substantially altered the magnitude or direction of the association. Similar consistency was observed for safety endpoints with at least three available studies (Supplementary Figures 13).
When restricting analyses to trials enrolling strictly resistant hypertension, the magnitude and direction of SBP reduction were unchanged, confirming that inclusion of uncontrolled-only trials did not materially influence pooled estimates.
Risk of bias assessment
In the risk of bias assessment, all included studies were rated as low risk of bias across all domains of the Cochrane RoB 2 tool.
The studies were judged to have low risk in the randomization process, adherence to interventions, completeness of outcome data, outcome measurement, and selective reporting, supporting high internal validity (Supplementary Figure 4).


In this systematic review and meta-analysis of five RCTs comprising 2,637 patients with resistant or uncontrolled hypertension, treatment with ASIs significantly reduced SBP by approximately eight mmHg compared with placebo, with consistent effects across individual agents and trials. This reduction is clinically meaningful, corresponding to an estimated 20–25% lower risk of major cardiovascular events when extrapolated from population level hypertension outcomes [1,18,19]. In parallel, ASI therapy was associated with predictable increases in hyperkalemia, hyponatremia, and hypotension, but without significant differences in all-cause mortality or decline in renal function.
The magnitude of reduction observed across agents was robust and coherent, even in studies employing distinct background therapies and diverse patient characteristics. These findings align with contemporary phase II and phase III trials, such as BrigHTN [8], TargetHTN [5], LaunchHTN [10] and the 2025 baxdrostat trial [11], which independently confirmed the antihypertensive efficacy of selective ASIs in real-world–like populations. Compared with earlier systematic reviews [12], the present study provides a more precise estimate of treatment effect by restricting inclusion to fully selective ASIs, focusing exclusively on resistant or uncontrolled hypertension, and incorporating the latest high-quality trial data. This addresses a key limitation of previous syntheses, which combined heterogeneous agents and populations and therefore could not offer definitive guidance for clinical practice.
Mechanistic considerations of ASIs strengthen the biological plausibility of their antihypertensive effects. Aldosterone excess contributes to sodium retention and plasma volume expansion, but also triggers vascular inflammation, endothelial dysfunction, oxidative stress, and tissue fibrosis. Inhibiting CYP11B2 at the site of aldosterone synthesis prevents activation of both genomic and rapid nongenomic pathways implicated in treatment resistance. Second-generation ASIs preserve cortisol physiology by minimizing off target inhibition of CYP11B1, overcoming the limitations of earlier molecules [20]. The ability to suppress aldosterone production upstream differentiates ASIs from mineralocorticoid receptor antagonists and provides a complementary therapeutic mechanism that may ultimately allow combination approaches in high-risk hypertensive patients [21].
Globally, hypertension affects more than 1.2 billion adults, and 10–20% of treated individuals meet criteria for resistant hypertension, defined as uncontrolled BP despite three or more antihypertensive agents, including a diuretic [1,18,19,22]. These patients exhibit persistently elevated cardiovascular risk and limited treatment options, with approximately a twofold higher incidence of adverse cardiovascular events compared with those achieving target blood pressure [19,22]. The magnitude of this unmet need underscores the rationale for innovative pharmacologic strategies beyond conventional Renin–Angiotensin–Aldosterone System (RAAS) blockade.
Aldosterone plays a central pathophysiologic role by promoting renal sodium retention, vascular remodeling, inflammation, and myocardial and renal fibrosis [20,21,23,24]. Traditional mineralocorticoid receptor antagonists (MRAs) such as spironolactone and eplerenone remain the recommended fourth line therapy for resistant hypertension. Still, they are often limited by hyperkalemia and endocrine adverse effects, particularly in patients with diabetes or chronic kidney disease [19,21,23]. In contrast, selective ASIs act upstream by inhibiting CYP11B2, the terminal enzyme in aldosterone biosynthesis, thereby reducing aldosterone synthesis at its source [21,25–27]. This mechanism differs fundamentally from receptor blockade and preserves physiologic glucocorticoid and androgen signaling.
Earlier first-generation ASIs, such as osilodrostat (LCI699), demonstrated proof of concept antihypertensive efficacy but were hindered by limited selectivity over CYP11B1, leading to cortisol suppression and off target effects [25–28]. Advances in medicinal chemistry have produced next generation molecules, most notably lorundrostat and baxdrostat, with markedly improved CYP11B2/CYP11B1 selectivity, minimizing cortisol interference while maintaining potent antihypertensive effects [21,23,27,29]. These pharmacologic refinements have facilitated the clinical translation of aldosterone synthase inhibition into latephase development programs.
Although pooled efficacy was similar for lorundrostat and baxdrostat, safety profiles showed subtle differences. Lorundrostat demonstrated a more consistent signal of hyponatremia and hypotension, whereas baxdrostat exhibited numerically higher—but still infrequent—episodes of hyperkalemia. These patterns are based on limited patient numbers and wide confidence intervals but may help guide early clinical decision making until more robust comparative data emerge.
Our results align with recent phase II and III trials, including Brig HTN [8], HALO [5], Target HTN [9], Launch HTN [10], and the 2025 NEJM trial by Flack et al. [11], which consistently reported SBP reductions of 7–11 mmHg among patients with resistant or uncontrolled hypertension. These findings support the reproducibility of ASI efficacy across diverse populations. Compared with a previous meta-analysis encompassing broader hypertensive cohorts [12], our study refines the evidence base by focusing exclusively on resistant and uncontrolled hypertension and by incorporating the most recent phase III data, yielding more clinically relevant and precise pooled estimates.
The observed adverse events were primarily biochemical and hemodynamic, consistent with the mechanism of aldosterone inhibition. Hyperkalemia arises from decreased potassium excretion in the distal nephron, while hyponatremia and hypotension reflect reduced sodium reabsorption and plasma volume contraction [20,21,23,24]. These effects were generally mild to moderate and predictable. Significantly, definitions of hyperkalemia and monitoring protocols varied modestly across trials, as outlined in Table 3, which may have influenced absolute event rates but did not alter the direction or consistency of the pooled risk estimates. Notably, the pooled cohort included patients with obesity (mean BMI 32.1 kg/m²) and diabetes (36%), both of which predispose to electrolyte disturbances and renal dysfunction. Current hypertension guidelines [1,19] and recent expert reviews [21,23,29] emphasize the importance of structured laboratory monitoring and optimization of background therapy to mitigate these predictable, mechanism based risks.
Beyond hemodynamic mechanisms, emerging translational data indicate that aldosterone excess contributes to vascular inflammation and fibrosis through immune modulation. Aldosterone promotes proinflammatory macrophage polarization, oxidative stress, and vascular collagen deposition, processes that may be attenuated by CYP11B2 blockade [24,30]. These mechanistic findings suggest that selective ASIs may exert vasculoprotective effects beyond blood pressure control, potentially complementing the organ protective benefits of nonsteroidal MRAs and Sodium Glucose 2 Transporter (SGLT2) inhibitors [20,21,23].
Subgroup analyses comparing individual ASIs should be interpreted cautiously. These analyses were not powered to detect differences between agents, particularly for safety outcomes with low event counts. Therefore, all subgroup comparisons are exploratory and hypothesis generating rather than confirmatory.
In contemporary treatment pathways, MRAs remain the guideline recommended fourth line option for resistant hypertension. ASIs may ultimately serve as an adjunct or alternative in patients unable to tolerate MRAs because of hyperkalemia, gynecomastia, or worsening renal function. Upstream aldosterone inhibition could offer complementary benefits when combined with MRAs, although this concept requires formal testing. As evidence grows, ASIs may occupy a niche role for high-risk patients with aldosterone driven hypertension, but integration into treatment algorithms must await results from longer and comparative trials.
Limitations
This meta-analysis has several limitations. Although large phase III studies were included, the overall number of available RCTs remains limited, and most had relatively short follow-up, limiting the evaluation of long-term cardiovascular or renal outcomes. Event counts for mortality and kidney endpoints were low, limiting the precision of these estimates. Heterogeneity in study inclusion criteria and in background RAAS blockade may have influenced electrolyte outcomes and reduced comparability across trials. Furthermore, publication bias was not formally assessed because fewer than 10 studies were eligible, and the absence of head-to-head comparisons with MRAs precludes definitive conclusions regarding comparative efficacy or tolerability.
Nonetheless, the consistent reductions in SBP across studies, together with the absence of significant statistical heterogeneity, support the robustness and clinical relevance of our findings.
Because no trials directly compared ASIs with MRAs, any suggestion of their role as a fourth line therapy should be viewed as preliminary. Larger head-to-head trials are needed before establishing their position relative to spironolactone or eplerenone in resistant hypertension algorithms.
In summary, ASIs represent a promising therapeutic advance for patients with resistant or uncontrolled hypertension. By directly suppressing aldosterone synthesis, these agents achieve clinically meaningful BP reductions while maintaining an acceptable safety profile characterized by manageable electrolyte disturbances. Collectively, these data support selective ASIs as an emerging fourth line or alternative option to MRAs, particularly for patients at risk of endocrine adverse effects. Larger, longer-term outcome trials are warranted to confirm these benefits and define their optimal role in hypertension management algorithms. Because fewer than 10 RCTs were eligible, formal statistical assessment of publication bias was not feasible. This limitation raises the possibility that the available evidence may overestimate treatment effects if negative or neutral trials remain unpublished.
| FREEMAN, 2023 | LAFFIN, 2023 | LAFFIN, 2025 | SAXENA, 2025 | FLACK, 2025 | |
|---|---|---|---|---|---|
| Trial phase | Phase II | Phase II | Phase IIb | Phase III | Phase III |
| Population | Resistant hypertension | Uncontrolled hypertension | Uncontrolled and treatment-resistant hypertension | Uncontrolled and treatment-resistant hypertension | Uncontrolled and treatment-resistant hypertension |
| Intervention | Baxdrostat | Lorundrostat | Lorundrostat* | Lorundrostat | Baxdrostat |
| Control | Placebo | Placebo | Placebo | Placebo | Placebo |
| Duration of study (Weeks) | 12 | 8 | 12 | 12 | 52 |
| Number of Patients | 275 | 200 | 285 | 1083 | 794 |
| Male Sex - n(%) | 153 (56) | 80 (40) | 172 (60) | 575 (53) | 494 (62) |
| Age, years | 62.3 (10.5) | 65.6 (10.2) | 60.4 (10.1) | 61.7 (10.5) | 61.2 (11.7) |
| BMI | 32.6 (5.2) | 31.1 (5) | 31.9 (5) | 32.8 (7) | 31.3 (6.2) |
| Baseline SBP, mmHg | 147.9 (12.4) | 141.6 (12) | 153.6 (12.2) | 148.4 (12) | 149.3 (9.3) |
| Baseline DBP, mmHg | 87.9 (6.7) | 81.1 (9.6) | 89.2 (9.4) | 87.3 (9.1) | 86.5 (10.5) |
| eGFR, mL/min per 1.73 m2 | 83.7 (19.5) | 79.6 (15.1) | 75.5 (18.4) | 91 (17.4) | 85.0 (18.1) |
| Diabetes n(%) | 105 (38) | 79 (40) | 119 (42) | 338 (31) | 303 (38) |
| >3 Background AHM- n (%) | 275 (100) | 90 (45) | 115(40) | 651 (60) | 579 (73) |
Data are expressed as mean (standard deviation), otherwise indicated.
AHM: Antihypertensive Medication; BMI: Body Mass Index; DBP: Diastolic Blood Pressure; eGFR: Estimated Glomerular Filtration Rate; NA: Not Availble; SBP: Sistolic Blood Pressure.
*Participants receiving two antihypertensive medications were assigned to olmesartan 2.5 mg/day or hydrochlorothiazide 25 mg/day; those receiving three to five antihypertensive medications were assigned to olmesartan 2.5 mg/day or hydrochlorothiazide 25 mg/day in combination with amlodipine 10 mg/day.
| Trial | Definition of Resistant vs. Uncontrolled HTN | Background therapy requirements | BP entry thresholds |
|---|---|---|---|
| Target-HTN | Uncontrolled HTN: SBP above target despite ≥2 antihypertensives | Stable antihypertensive regimen ≥4 weeks | SBP ≥140–180 mmHg |
| Launch-HTN | Resistant HTN: uncontrolled on ≥3 drugs including a diuretic | Triple therapy required (ACEi/ARB + CCB + diuretic) | SBP ≥140–180 mmHg |
| BrigHTN | Resistant HTN | ≥3 antihypertensive drugs including a thiazide-type diuretic | SBP ≥140–179 mmHg |
| NEJM Baxdrostat 2025 | Resistant or uncontrolled HTN | ≥2–3 standard antihypertensive agents | SBP ≥130–180 mmHg |
| BI 690517 | Uncontrolled and treatment-resistant HTN | Standardized regimen including ARB (olmesartan) + thiazide-type diuretic ± CCB (RAAS inhibitor required) | SBP ≥130–180 mmHg |
| Trial | Hyperkalemia definition | Absolute rate | Placebo rate | Maximum dose rate |
|---|---|---|---|---|
| Target-HTN | K⁺ ≥5.6 mmol/L | 18 / 164 (11.0%) | 2 / 36 (5.6%) | 9 / 61 (14.8%) |
| Launch-HTN | K⁺ ≥5.6 mmol/L | 77 / 808 (9.5%) | 5 / 270 (1.9%) | 33 / 270 (12.2%) |
| BrigHTN | K⁺ >5.5 mmol/L | 10 / 205 (4.9%) | 1 / 69 (1.4%) | 3 / 67 (4.5%) |
| NEJM Baxdrostat 2025 | K⁺ >5.5 mmol/L | 48 / 530 (9.1%) | 7 / 264 (2.7%) | 31 / 266 (11.7%) |
| BI 690517 | K⁺ >6.0 mmol/L | 12 / 188 (6.4%) | 0 / 94 (0.0%) | 7 / 96 (7.3%) |
Selective aldosterone synthase inhibitors represent a promising therapeutic advance for patients with resistant or uncontrolled hypertension. By directly suppressing aldosterone production, these agents achieve clinically meaningful reductions in blood pressure with a predictable and generally favorable safety profile. This meta-analysis provides the most UpToDate and methodologically rigorous synthesis of available evidence supporting their antihypertensive efficacy. However, the long-term cardiovascular and renal benefits of selective aldosterone synthase inhibition remain to be established, and their optimal role relative to mineralocorticoid receptor antagonists is not yet defined. Head-to-head, adequately powered outcome trials are needed before selective aldosterone synthase inhibitors can be recommended as alternatives or adjuncts to established fourth line therapies.
Funding: The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Competing interests: All authors certify that they have no affiliations with or involvement in any organization or entity with any financial or nonfinancial interest in the subject matter or materials discussed in this manuscript.
Author contributions: All authors contributed to the study’s conception and design. Material preparation, data collection, and analysis were performed by Mariana Marques Seixas, Railla Raquel Albino dos Santos Silva, Pedro Gomes Batista, Lucas Diniz da Conceição, Juliana Martins Giorgi. The first draft of the manuscript was written by improved by and reviewed by All authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Ethics approval: Not applicable. This is a meta-analysis. The Sirio Libanes Research Ethics Committee has confirmed that no ethical approval is required.
Data availability statement: The data used in this meta-analysis were extracted from publicly available sources, including published observational and randomized controlled trials. All relevant data supporting the findings of this study are included within the manuscript and supplementary materials. Due to the nature of this analysis, no new primary data were generated. Additional details can be made available upon reasonable request to the corresponding author.
