-
Email [email protected]
-
Address 848 N. Rainbow Blvd. #5486 Las Vegas, NV 89107, USA
Leumit Health Care, Internal Medicine and Cardiology, Hebrew University, Jerusalem, Israel.
*Corresponding author: Ilia Davarashvili
Senior Cardiologist, Hebrew University, Jerusalem, Israel.
Tel+972548360613;Email ID: [email protected]
Received: Mar 13, 2026
Accepted: Apr 07, 2026
Published Online: Apr 14, 2026
Journal: Annals of Cardiology
Copyright: Davarashvili I © All rights are reserved
Citation: Davarashvili I. Post coronavirus remote myocarditis: Case report and review of the literature. Ann Cardiol. 2026; 3(1): 1018.
Severe acute respiratory syndrome is the new coronavirus responsible for the coronavirus disease 2019 (COVID-19), which was declared a global public health emergency by the World Health Organization on March 11, 20 [1-3]. As for COVID-19 updated registry, 422 million confirmed cases have been reported globally to for February 2022, with 5 million deaths worldwide.
The main presentation of COVID-19 disease is characterized by acute respiratory distress syndrome and atypical pneumonia [1]. Emerging studies demonstrated the harmful effects of SARS- CoV-2 on the Cardiovascular (CV) system, such as myocardial injury, which is associated with myocardial inflammation and damage [2]. It is suggested that heart injury caused by COVID-19 infection might be an important cause of severe clinical phenotypes or adverse events in affected patients [3]. Myocardial damage is closely related to the severity of the disease and even the prognosis in patients with COVID-19 [3]. In addition to disorders that are caused by COVID-19 on the cardiovascular system, more protection should be employed for patients with preexisting Cardio Vascular Disease (CVD) [3]. Hence, it is very important that once relevant symptoms appear, patients with COVID-19 be rapidly treated to reduce mortality [3]. Prior viral illnesses, including Middle East Respiratory Syndrome Coronavirus (MERS-CoV), have been associated with myocardial injury and myocarditis with troponin elevation, thought to be due to increased cardiac physiologic stress, hypoxia, or direct myocardial injury [4-14]. Several studies reported that myocardial injury with an elevated troponin level may occur in 7-17% of patients hospitalized with COVID-19 & 22-31% of those admitted to the Intensive Care Unit (ICU) [15- 17].
Acute myocarditis presents across a variable range of clinical severity and is a significant diagnostic challenge in the COVID-19 era. Patients with COVID-19 can present with chest pain, dyspnea, dysrhythmia, and acute left ventricular dysfunction [15-19]. In patients with myocarditis and myocardial injury, serum troponin values will be abnormal. The Electrocardiogram (ECG) can demonstrate a range of findings, in some cases mimicking Acute Coronary Syndrome (ACS) [20].
Mostly, reported cases of acute myocarditis after COVID-19 disease were reported within three months after initial presentation [21].
Keywords: Chest pain; Coronary artery disease; Exercise stress test; Cardiac MRI; Myocarditis; COVID-19; Case report.
We present a case of a 54 years-old female patient with known family history of ischemic heart disease, which presented at clinics with chest pain and palpitations. Echocardiography showed mild ventricular dysfunction (EF=50%) with no segmental wall motion abnormality, normal RV size and function, normal LA and RA size, trace MR, PA pressure within normal limits.
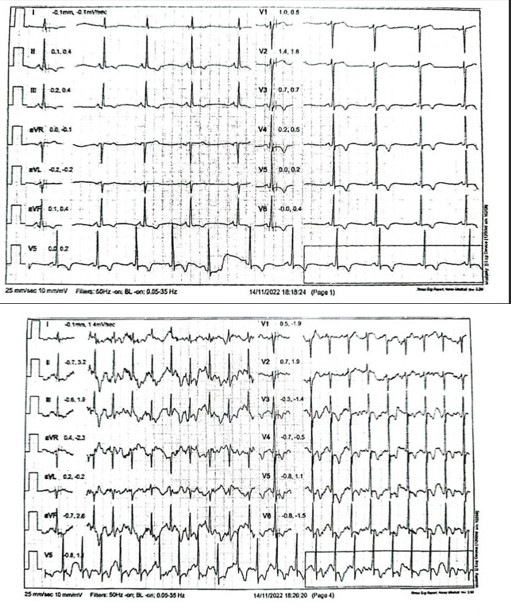
The patient was referred to routine follow-up exercise stress test. Vital signs were normal before starting the test. ECG at rest showed sinus rhythm with T wave inversion in leads V2-6, II, AVF. On exercise normal heart rate response seen with very deep T inversions (Figure 1). The test was ended due to chest pain at 82% target heart rate; maximal heart rate achieved was 137 bpm. Blood pressure has raised from 110/60 to 130/60 mm Hg.
The blood tests showed: Normal WBC count, liver and kidney functions. Slight elevation of ESR 39 mm/h (normal range 2-30), CRP of 24.6 mg/L (normal range 0-5).
It was decided to perform coronary angiography which demonstrated normal coronary arteries.
Heart MRI was performed with the criteria fulfilling the diagnosis of remote myocarditis.
Myocarditis is described as inflammation of the heart muscle, leading to damage in the absence of ischemia [22,23]. Viruses have been suggested to be a significant etiology for myocarditis with a wide variety of causative agents including, but not limited to, adenovirus, parvovirus B19, Epstein Barr virus and cytomegalovirus [23-26]. Now, recent evidence suggests the SARS-CoV-2 virus may also be a significant infectious agent for myocarditis. The proposed pathophysiology of viral myocarditis is a combination of direct cell injury and immune-mediated cell death [22]. Early in the development of viral myocarditis high rates of viral replication leads to direct cardiomyocyte injury [27]. The damaged cells, and proteins released from them (such as cardiac myosin), activate toll-like receptors and inflammasomes, leading to the release of pro- inflammatory cytokines [28,29]. As time progresses, these pro-inflammatory cytokines recruit immune cells, including natural killer cells, macrophages and T-lymphocytes, to the myocardium. These cells are involved in immune-mediated myocyte injury [27]. Moreover, Interleukin (IL)-1β and IL-17 cause cardiac remodeling and fibrosis, which eventually leads to dilated cardiomyopathy and heart failure [30,31]. Myocardial fibrosis leads to a disruption in the conduction system, leading to an increased risk of developing arrhythmias [32].
It was found that number of diffusely distributed CD68 + cells in hearts of patients with COVID-19 is increased, compared to those with typical myocarditis and control groups. Fox et al. hypothesized the difference in immune cells on histology suggest COVID-19 myocarditis is a distinct inflammatory process separate from typical viral myocarditis [33]. Two theories describing the inflammatory process were proposed. First, SARS-CoV-2 can infect endothelial cells within coronary vessels, leading to the migration of macrophages to these areas, causing the activation of complement and apoptosis [33]. Second, the inflammation can lead to thrombus formation in the coronary vessels leading to ischemic myocardial injury [33].
Systemic inflammation may also play a role in the development of COVID-19 myocarditis. IL-6 is a cytokine implicated in the pathophysiology of myocarditis, recruiting inflammatory cells to the myocardium [34]. IL-6 is also a primary mediator of the cytokine storm, a life-threatening condition seen in some patients who have developed COVID-19, which is characterized by extreme increases in pro-inflammatory cytokines and an uncontrolled immune response [34,35]. This systemic inflammation can further increase the risk of thrombus formation within coronary vessels due to activation of platelets and high levels of clotting factors (including factor V and VIII) [36,37]. It is also possible that the cytokine storm may lead to exacerbation of established myocarditis and further myocardial injury [38]. Furthermore, myocardial injury may be exacerbated by hypoxia of the myocardium due to increased oxygen demands in the setting of infection, which cannot be met due to the presence of pneumonia of acute respiratory distress syndrome [39].
Unfortunately, the incidence of COVID-19-induced myocarditis is unclear [40]. The true incidence of COVID-19 myocarditis may be underestimated, as some patients may be asymptomatic or have minor symptoms. Puntmann et al. studied 100 patients who had recently recovered from severe COVID-19 and found 78% exhibited cardiac involvement on cardiac magnetic resonance imaging (cMRI), with 60% found to have ongoing inflammation [41]. Published evidence does show that the myocardial involvement increases mortality in patients hospitalized with COVID-19 [42].
A systematic review and case series demonstrated that patients with cardiovascular comorbidities were more at risk at developing COVID-19 myocarditis [43,44]. Black, Asian and minority ethnic (BAME) groups may be more seriously affected of cardiovascular disease among these groups [45-49].
An important group to be vigilant of are those who compete in competitive sports as myocarditis is associated with sudden cardiac death in athletes [50]. The cardiac involvement of COVID-19 is underestimated due to asymptomatic patients in this group of patients [51]. Athletes who have recovered from COVID-19 and are returning to sports should receive cardiac testing, including cMRI, to screen for any active myocarditis or the previous cardiac injury [52].
Classic presentation of myocarditis is analogous to heart failure, with symptoms of dyspnea, orthopnea and chest pain maybe present [53]. However, clinical presentations of patients with COVID-19 myocarditis can vary from patient to patient. Some patients have relatively mild presentations such as cough, fever and dyspnea [32,54-57]. These symptoms may be due to COVID-19 itself and not the myocarditis. Therefore, some patients may have a silent presentation of COVID-19 myocarditis [32]. Some patients may present with chest pain which may or may not be described as a pressure [57-59]. In one report this chest pain was present without fatigue, cough or dyspnea [60]. Some patients may also present with palpitations alongside their other symptoms [57,61].
C-Reactive Protein (CRP), Lactate Dehydrogenase (LDH) and White Cell Count (WCC) have been shown to be raised in patients with COVID-19 myocarditis [57-59]. Raised cardiac enzymes (e.g., troponin) and N-Terminal pro-B-type Natriuretic Peptide (NT-pro-BNP) have also been noted in COVID-19 myocarditis [59]. However, some patients with COVID-19 myocarditis may not have a raised troponin, meaning a normal troponin does not rule out myocarditis [59].
Most changes are non-specific and can include sinus tachycardia (the most common change), ST segment elevation/ depression, T wave inversions, tachy/bradyarrhythmia and QT prolongation [59]. Echocardiography can be useful to rule out other causes of heart failure, such as valvular or congenital causes [61].
cMRI has a high sensitivity for diagnosing myocarditis and is therefore the best noninvasive test [62]. The Lake Louis criteria should be used when interpreting cMRI images [63]. This criterion uses a combination of T2-weighted images, early gadolinium enhancement and late gadolinium enhancement to detect myocardial edema, hyperemia and myocardial necrosis and fibrosis, respectively [63-65]. cMRI has shortcomings as it is not possible to distinguish whether the inflammation is caused from an autoimmune response to the virus or from viral infection of the myocardium [63].
Treating myocarditis involves the management of both the myocardial inflammation and the complications that may arise from it. Intravenous Immunoglobulins (IVIG) have been studied for their efficacy in treating viral myocarditis. IgG, IgA and IgM immunoglobulins have anti-inflammatory effects, while neutralizing and facilitating the clearance of pathogens from the myocardium [66]. However, in cases of suspected myocarditis with no biopsy proof of viral infection, use of immunoglobin therapy showed inconsistent results [67]. Hu et al. used a combination of glucocorticoid and immunoglobulin treatment to successfully treat COVID-19 myocarditis [68]. A meta-analysis revealed that the use of IVIG to treat acute myocarditis significantly reduced mortality, while improving left ventricular ejection fraction [69]. Moreover, the effect of by COVID-19-induced myocarditis, due to a greater prevalence IVIG was even more noticeable in patients with fulminant myocarditis where it showed to significantly increase survival rates of this life-threatening condition [69]. The evidence for use of corticosteroids to treat COVID-19 myocarditis is not as clear. The use of the corticosteroid, prednisolone, may be effective in treating viral myocarditis in the absence of viral [70]. It is thought that the use of immunocompromising medication, such as corticosteroids, may worsen acute myocarditis where viral replication is present [71]. A systematic review by Sawalha et al. revealed the use of corticosteroids showed improved outcomes among patients with COVID-19 myocarditis [72]. On the other hand, other studies show the use of corticosteroid therapy does not reduce mortality in patients with viral myocarditis [73]. Tocilizumab, which is an anti-IL-6 receptor monoclonal antibody, was trialed with the combination of the anti-viral, favipiravir, to treat COVID-19 patients who had developed cytokine storm [74]. The trial found that the combination of Tocilizumab and favipiravir significantly reduced inflammation caused by cytokine storm [75]. As COVID-19 myocarditis may be exacerbated by cytokine storm, the use of this combination therapy may provide positive outcomes [38]. Although there is evidence to show the efficacy of IVIG in the treatment of viral myocarditis, more research is needed to assess the effects on COVID-19 myocarditis specifically. Dexamethasone, a corticosteroid, is currently used in the management of COVID-19. Therefore, research into assessing the efficacy of Dexamethasone may reveal if current treatment is sufficient or if patients who develop COVID-19 myocarditis require extra anti-viral/anti-inflammatory treatment.
Patients who present with cardiogenic shock due to fulminant myocarditis need further management. For patients with cardiogenic shock, the use of inotropic agents, such as dobutamine, and mechanical support, including intra-aortic balloon pumps or Impella systems, can be used to maintain blood pressure [61,62].
COVID-19 myocarditis is a significant complication of SARS- CoV-2 infection which can worsen the prognosis for patients. While some cases may be insignificant or asymptomatic, it is likely clinicians will come across cases which are more severe and require prompt treatment. Therefore, it is imperative to recognize how to diagnose and treat this condition. If possible, it is a good idea to carry out serial troponins and ECGs to monitor for any development of myocarditis or other myocardial injury. As the symptoms for myocarditis can be non-specific and can overlap with the respiratory symptoms of COVID-19, it may be hard to diagnose this condition. It is important to have a low threshold to work up a patient, as initial tests are relatively inexpensive. Further testing should be used for patients with evidence of myocardial injury on initial work up, these include echocardiography, cMRIs and EMB. Clinicians should be vigilant for any signs of heart failure or arrhythmias, as these could be the life-threatening signs of fulminant myocarditis. While no definitive treatment for COVID-19 myocarditis has been published, the combination of IVIG and corticosteroids shows promise to reduce mortality, particularly in the case of fulminant myocarditis.
In this report we presented a case of remote myocarditis mimicking angina with ischemic changes on ECG. Coronary angiography demonstrated normal coronary arteries. This female patient recovered from COVID-19 infection year before this admission with no other concurrent illnesses during this period. As seen on MRI and blood tests showed the inflammation was still undergoing besides distant active viral disease year before showing remote immunity as an active part of COVID-19 myocarditis.
