-
Email [email protected]
-
Address 848 N. Rainbow Blvd. #5486 Las Vegas, NV 89107, USA
1Leumit Health Care, Hebrew University of Jerusalem, Israel.
2Shaare Zedek Medical Center, Jerusalem, Israel.
*Corresponding author: Ilia Davarashvili
Senior Cardiologist, Hebrew University, Jerusalem, Israel.
Tel: +972548360613;Email ID: [email protected]
Received: Mar 13, 2026
Accepted: Apr 10, 2026
Published Online: Apr 17, 2026
Journal: Annals of Cardiology
Copyright: Davarashvili I et al. © All rights are reserved
Citation: Davarashvili I, Asher E. A retrospective review of the population of patients after angioplasty on venous grafts and review of the literature. Ann Cardiol. 2026; 3(1): 1019.
In many patients undergoing Coronary Artery Bypass Graft surgery (CABG), venous Saphenous (SVG) is used in addition to the arterial grafts. Treatment of degenerated and occluded venous graft is complex and challenging. Angioplasty on occluded venous bypass involves a high rate of complications (such as massive distal embolization).
Objectives: To review the demographic data, risk factors, outcome and complications of SVG’s use in CABG surgery and on this basis to build an algorithm for optimal treatment.
Methods: A retrospective study of patients who underwent angioplasty for SVG’s during 2005-2015 in a tertiary care hospital. Patients were divided into two groups: 2005-2009 (group A) and 2010- 2015 (group B) and the comparison was performed according to the demographic data, risk factors, time from CABG, as well as angiographic features.
Results: Among the 238 patients, 226(95%) were male, mean age 68±22 y, 74.4% suffered from hypertension, 56.3% suffered from diabetes mellitus, 17.2% suffered from chronic kidney disease, 99% had a history of previous myocardial infarction, 62% patients were admitted due to ACS. Distal protection devices were used in only 31(22%) patients.
Intervention was performed mainly on right and circumflex coronary arteries. Contrast amount was used in a less amount in group B (186 vs 137 ml, p=0.0018, respectively). There was more frequent use of covered stents in group B (18.8% vs 2.1%, p=0.003, respectively), as was the use of protection devices (36.4% vs 9.5%, p=0.0002).
Conclusion: The progression of the technologies and mainly the use of protection devices lowered the rate of complications while intervention on SVGs. This also was reflected in the lesser amount of contrast material used and kidney injury secondary to it. It has been observed that over the years there has been a tendency to treat more severely ill patients with longer time since surgery (“older" grafts).
Coronary Artery Bypass Graft surgery (CABG) has been performed for over four decades in millions of patients worldwide and is well known today. Despite increased experience and use of arterial grafts for bypass in recent years, not so few venous grafts have been used. As a result, the disease of the venous graft (saphenous vein graft disease-SVGD) continues to be a leading cause of symptomatic coronary artery disease after this surgery and usually occurs approximately 5-10 years after surgery [1].
In the first year after surgery, the venous grafts remain patent in about 80-85%, with an average patency range of 8-9 years [2,3], with a 50% reduction in the rate of long-term patency thereafter. Repeated surgery is not justified in most cases, therefore, a catheterization intervention is in most cases the preferred strategy for revascularization.
Numerous studies and meta-analyzes have shown a pathophysiological and clinical difference between diseases of the venous grafts and coronary arteries. The correct choice of the patient, the initial treatment, the stent type, and the use of various aids for revascularization such as the protection device have the effect of achieving optimal results both in the immediate and in the long term. However, even under this treatment, SVGD remains a significant problem with a rate of 89% graft occlusion in the first year after surgery, and of up to 61% about 10 years thereafter [18].
In the Database Unit of the Hadassah Hospital, there were 238 patients who had undergone intervention on venous grafts during the last decade. They were divided into two groups: 2005 to 2009 (Group A) and the second group (Group B) - from 2010 to 2015 and the comparison was performed according to demographic data (age, sex), risk factors (hypertension, diabetes mellitus, kidney failure), time from CABG, as well as angiographic features, severity of the coronary disease, amount of delivered contrast material and final result (according to resumption of flow) (Table 1).
| All | Group A | Group B | p-value | |
|---|---|---|---|---|
| n=238 | ||||
| Age (years, mean±SD) | 68±22 | 67±21 | 68±21 | N |
| Female gender (%) | 5.0 | 4.7 | 5.6 | N |
| Hypertension | 74.4 | 77.9 | 68.5 | N |
| Diabetes Mellitus | 56.3 | 53.7 | 60.7 | N |
| Prior Myocardial Infarction | 99.2 | 98.6 | 98.9 | N |
| Congestive Heart Failure (data in 65%) | 91.5 | 83.1 | 98.8 | N |
| Renal failure | 17.2 | 19.5 | 13.5 | N |
| Clinical presentation | ||||
| Stable angina | 38.0 | 40.4 | 33.8 | N |
| ACS | 62 | 59.6 | 66.2 | N |
| Catheterization features | ||||
| Percentage of all angioplasties | 5.5% | 4.3% | ||
| Severity of coronary disease | 92.6 | 83.1 | 98.8 | N |
| TIMI flow 2/3 | 75.0 | 81.2 | 67.8 | N |
| Balloon dilatation | 59.5 | 57.2 | 63.1 | N |
| Integrilin | 6.3 | 8.0 | 7.0 | N |
| Nitroglycerin | 9.2 | 13.0 | 9.0 | N |
| BMS | 77.5 | 80.3 | 58.8 | N |
| Covered stents | 4.3 | 2.1 | 18.8 | 0.003 |
| Protection device | 22.1 | 9.5 | 36.4 | 0.0002 |
| Good angiographic result | 93.7 | 95.9 | 91.0 | N |
| Contrast amount (mean, ml) | 174.8 | 187.6 | 136.7 | N |
| Culprit lesion | ||||
| LAD | 21.0 | 21.9 | 19.3 | N |
| RCA | 37.1 | 32.9 | 44.6 | N |
| CX | 41.9 | 45.2 | 36.1 | N |
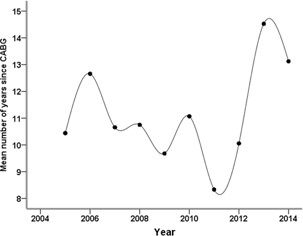
It was found that most of the population were men (95%), had previous MI, higher evidence was found of diabetic patients during the later years but with no statistical significance, there was a low of chronic kidney disease (17%) in both groups, there was a slight longer period after CABG before the interventions (10 vs 14 y).
62% percent of the patients were admitted for ACS syndrome.
The severity of the disease (assessed by the length of the lesion and the distal flow) was assessed to be at least moderate in 83% of the population with no difference between the groups.
The use of protection devices was of low rate (13%) in the general population, 9.5% in the early group and 36.4% in the later one (p=0.0002).
There was no difference in the rate of post-dilatation and use in vasodilatators.
The intervention was performed on similar coronary arteries and the lesser extent on the LAD lesions, supposedly because of the LIMA graft. There was more frequent use of covered stents in the later group (2.1% vs 18.8%). Good flow was achieved in both groups (95%).
The larger amount of contrast material was used in the earlier group (186 vs 137 ml).
There was a low rate of complications and death during the one-year follow-up and the most obvious reason is the retrospective data analysis.
The antiagregant treatment the patients were discharged was the combination of aspirin and Plavix (80 vs 73% in the early and later groups). The lesser extent of this combination in the later years was mostly explained by the use of newer antiaggregants (Ticagrelor and Prasugrel).
Over the years, the development of technology and the experience gained in invasive treatment approaches have raised the success rate to more than 90%. Catheterization and intervention on venous grafts currently accounts for 5.7% of all therapeutic catheterizations [4].
Venous Graft Failure (VGF) has many factors, both clinical and surgical [5-9]. A study examining the factors that increase the incidence of venous graft failure found that long surgery duration and poor quality of the target artery were variables associated with an increased risk of venous bypass failure [3,4].
Further studies have shown additional characteristics such as patient age, female gender, heart failure, and hypercholesterolemia as predictors of venous graft failure [10- 12]. Surgical variables such as the preservation temperature of the venous graft, the presence of multiple anastomoses, damaged distal portion of the vessels, and narrowing of the target artery were also possible predictors of VGF. However, it should be remembered that these analyzes were performed at a time when antiagregant therapy was less common [13-15].
In terms of long-term venous thrombosis, accelerated fibrosis and advanced arterial atherosclerosis are the major cause of acute thrombosis [46,19]. Compared with the angioplasty on native arteries, intervention on venous grafts is more challenging and involves a higher rate of periprocedural acute coronary infarction due to atheromatotic and thrombotic tissue along the graft [20]. The most common immediate complication of venous graft angioplasty is distal embolization, probably due to friable plaque mixed with clot. Such an embolization may result in no flow or slow flow (slow flow phenomenon), and these can cause acute and extensive ischemia with ST segment changes with an acute coronary syndrome rate about 30% [21- 23,36]. There was no correlation between the anatomic size of the graft and its effect on distal embolization, and this due to release of inflammatory factors and higher left ventricular insufficiency [36,37].
Venous graft occlusion may be manifested in various forms increased heart enzymes, acute heart failure, arrhythmias, stable angina, acute coronary syndrome without ST elevation (NSTE), with ST Eelevation (STE), and cardiac arrest [16,17,57,58]. A stress test with or without additional imaging may arise suspicion of ischemia but does not differentiate between a native artery or graft disease [60]. Angiography is the primary and most accurate means of diagnosis, which will determine the need and possible profit from re-vascularization. One of the common approaches is an intervention only in cases of proximal Left Anterior Descending artery (LAD) or multiple graft disease [61].
Venous graft disease is a leading cause of death after bypass surgery. Three common approaches are well known conservative, interventional (catheterization) and repeat coronary artery bypass surgery [46].
A therapeutic approach to anticoagulation in patients undergoing catheterization on venous grafts has changed significantly since the 1990s. The treatment then included, aspirin, dipiridamole, and warfarin along with heparin in high-risk patients, and now the treatment is mainly potent antiagregants [64]. In various studies, routine use of IIb-IIIa inhibitors failed to decrease distal embolization rate with significant increase in bleeding risk compared to placebo [65-67].
Two major issues remain disputable in patients undergoing coronary bypass surgery [93]. The first is what is the preferred location for intervention - it is known that intervention on friable lesions of venous grafts causes a high rate of recurrent stenosis and even the formation of new lesions leading to Target Vessel Failure (TVF) [94-97]. On the other hand, there are few retrospective studies showing the algorithm for selection of the preferred lesion for intervention on a native artery or venous graft [98,99].
The second issue what is the preferred stenting for venous grafts [47,93]. It is clear, stenting is the preferred strategy for angioplasty [100]. Short-term outcomes for balloon angioplasty were not good and longer-term outcomes were even more disappointing with recurrent stenosis increasing to 70% at 6 months [3].
The use of the stents was compared with a balloon angioplasty in the SAVED TRIAL, an improved outcome was shown both in the immediate and long term, i.e., a reduction in Major Adverse Cardiac Events (MACE) [47].
After demonstrating the priority in using the stents, they became an integral part of the procedure, but the recurrence rate of stenosis remained fairly high. The preferred ones were DES due to reduced need for repeated interventions and MACE, but mortality rates remained similar in both groups [48-50].
In a study performed in the United States, the use of a DES was better than that without, and there was a further increase in the rate of use of the coated stents since 2009 [42,44,45,62]. Periprocedural side effects were less in a DES group (4.2% P <0.0015.9%, vs.) [26,33,40,43].
Another big study in 80 patients with intervention on venous grafts using standard stents and Paclitaxel-covered stents did not show difference in mortality rate between groups, but using DES reduced need for repeated interventions and acute coronary events during average follow-up of 34 months [42].
PTFE-coated stents may also be useful while intervention on venous grafts preventing distal embolization, but few of the studies demonstrated this [51-54].
Two other types of drug-coated stents - SESAME STENT and MGUARD STENT - did not produce optimal clinical results due to lack of long-term follow-up [55,56].
Another debate asked was whether the preferred approach is the intervention on several lesions in the same venous graft or several grafts during the index procedure, but in one large study no difference was found [63].
What are the possible explanations for higher death rate in the BMS group? According to DELAYED-RRISC TRIAL, mortality in the standard stent group compared to SES was higher and may be secondary to the shorter antiagregant therapy in two to three months [43].
Several possible explanations were presented as causes of MACE using drug-eluting stents: less stable lesions than in normal arteries, a tendency towards atherosclerosis, regional thrombotic and inflammatory response, mainly due to the drug and polymers with the endothelium. Another hypothesis is the creation of late aneurism and extensive inflammation adjacent to the artery wall [3,92,97].
Regarding the second issue of the preferred stents, studies on drug-eluting stents are limited in terms of population size and length of follow-up, with the exception of two studies - RRISC and SOS [92]. Results of angioplasty using DES on native vessels showed reduced mortality and for target artery disease during follow-up of 27 months (p<0.001). Therefore, there was no difference between normal or venous implant grafting [92]. There are many reasons for this: a larger diameter of a standard stent, a thrombotic and inflammatory response while using DES, and the progression of graft disease as a more substantial cause than re-stenosis [29].
In the absence of collaterals, the distal blockage expressed in stasis and the formation of a thrombus is a well-known phenomenon in intervention on venous grafts [57]. So it is always necessary to consider whether intervention on venous graft is beneficial and if not if the intervention on native artery should be performed [57]. If this is not possible, conservative treatment can be tried if there is no harm to quality of life or high-risk for myocardial infarction [57].
In the absence of many randomized studies on venous graft intervention, the question is what is the optimal therapeutic approach? According to today’s experience a reduction in the MACE rate can be achieved in several ways:
1. Careful selection of venous graft lesions to prevent interference on diffuse disease.
2. Using the EBD (distal occlusion balloons, distal filters, or proximal occlusion balloons).
3. Using stents with a smaller diameter.
4. Preliminary preparation with coronary vasodilation [34,59].
It is known that the frequency of perforation while intervention on venous graft is common and especially with the presence of aneurysms [68,69]. They occur at a frequency of about 1%, but there are no major studies in the field [70]. The “No Flow Phenomenon" is known in angioplasty for venous grafts and occurs in about 20% of cases [71]. Patients with this condition are usually older and less likely to have symptoms of angina [77]. There is no difference by gender or cardiovascular risk factors [78].
There is big clinical significance to the NO-REFLOW phenomenon, which is associated with increased mortality and acute coronary syndromes, left ventricular dysfunction, ventricular arrhythmias, and premature heart Failure (CCF) [79].
A number of researchers have proposed a classification of the “NO-REFLOW" phenomenon according to the “structural" and “functional" clinical characteristics [80]. The structural damage is defined as small blood vessel disease within the necrotic muscle, and the functional is defined as narrowing of the blood vessel affected by the spasm with/without embolization and this subgroup is more common in humans [89,81]. The mechanism of the phenomenon is multi-factorial and causes such as vasoactive substances, endothelial injury, oxidative inflammation and stress [72,73]. If the phenomenon “NO-REFLOW" occurred, the need for hemodynamic support (pressors, IABP), optimal oxygenation and the use vasodilators is extremely important [83].
The use of vasodilators for the first was performed in 1989 with the a good outcome using papaverine in a single patient [84]. The old studies have shown that nitrates and thrombolytic therapy were ineffective [75]. Today, there is insufficient data on pre-medication for prevention of thrombotic events in venous grafts [3].
The reaction to pharmacological substances is highly variable. For example, primary angioplasty in STEMI is very resistant to this treatment [83]. In contrast, the prevalence of NO-REFLOW is more common in venous grafts, but they respond better to pharmacological expansion like adenosine and verapamil [78,79,85-87,90].
Nitric oxide is a potent vasodilator [82]. Compared with nitrites (eg, nitroglycerin), nitroprusside is a direct nitrate derivate but was not tested broadly in “NO-REFLOW" phenomenon [82]. In one of the largest prospectively trials, nitroprusside was selective injected to the target vessel, distally to narrowing [91]. The restoration of the TIMI flow and ST segment elevation resolution was similar to placebo group [91]. It is important to note that the need for target vessel revascularization, acute MI and mortality rates were significantly less than in placebo group, but no significant improvement in coronary flow was seen [91].
Embolic protection devices
The advanced technologies using EPD are promising to prevent severe coronary side effects [82]. The use of EPD lowered a rate of acute MI during angioplasty on venous graft from 20% to less than 10% [47].
American College of Cardiology/American Heart Association PCI guidelines clarified and recommended the use of EPD during intervention on venous grafts [67]. But their use is not widespread and due to the ACC-NCDR registry is about 22% for venous grafts [67].
Since 2002, 4000 patients have been included in different studies on EPD [30-32]. One of them included 150 patients who have undergone CABG and a comparison was made between populations using EPD and those with direct intervention [26]. The EPD reduced the incidence of perioperative events to about 40% [27,38,39]. Despite the lower incidence of side effects in high-risk patients the cost-effectiveness is not substantial [28,29]. In this study the age of graft was older (9.23±0.08 vs 8.59±3.74), and there was no close association between the age of the bypass and side effects [27]. In the EPD group, most of them were males (86.4%) and older than in the direct intervention group [26].
Some factors including thrombus and aging of graft were described as possible causes of complications during angiographic intervention on venous grafts without EBD. Notably, there was no association between the side effects and the aging of the graft, thrombus or other angiographic characteristics, and no MACE indicators were observed. The MACE was observed at 17.2% in the direct intervention group and only 9.1% in the EPD group (P=0.53). The use of BMS was common in both groups (81.5% and 90%, respectively) but with no statistical significance (P=0.3). Still not clear if the right choice is using EPD or direct stenting. For MACE prevention, the choice falls on the use of EPD, although quite many operators prefer direct stenting because of both cost-effectiveness and accessibility [26,34].
We understand that the no-reflow phenomenon is a sign of prolonged and extensive ischemia as well as left ventricle dysfunction [82]. The most important is to prevent this, and to remember the differential diagnosis with coronary dissection, coronary spasm and acute thrombosis [3,74]. The use of protection devices gives a wider opportunity to treat this kind of lesions besides vasodilators like nitroglycerin [82].
In many patients with ischemic heart disease requiring revascularization by Coronary Artery Bypass Graft surgery (CABG), Saphenous Vein Graft (SVG) venous implant is frequently used in addition to the arterial ones. The venous grafts fall tend to be occluded in the higher rate than the arterial ones with need for revascularization after 5-10 years after the coronary bypass surgery.
Venous graft stenosis may be manifested in the wide range, including sudden onset of heart failure, arrhythmia, stable angina, acute coronary syndrome without ST and cardiac arrest.
The treatment of degenerated venous graft is complex and challenging. Few patients will undergo reoperation and a significant portion will be treated with a catheterization. Venous graft angioplasty comes along with a high rate of complications (such as massive distal embolization) and therefore the operator has to plan the procedure in details (with many technologies and utilities available for it).
Previous studies have examined the use of Bare Metal Stent (BMS), drug eluting stent - DES (or covered or mesh covered stent). The dispute has not yet been resolved.
We retrospectively examined a cohort of a population undergoing angioplasty for venous grafts over the past decade (from 2005 to 2015) at Hadassah Medical Center, Jerusalem.
The results showed that most of the patients are male, have diabetes and a more prevalent morbidity in recent years, most patients suffer from hypertension and mild to moderate heart failure. Most patients have ischemic heart disease prior to the index admission. There has been an increase for years after “bypass surgery" may be explained by higher rate of use of arterial grafts and advanced surgical technologies. Approximately 62% of patients were admitted with an ACS image and the rest performed electively based on a stress test (including mapping) or stable-angina clinics. This ratio has been maintained for years.
More than 90% of the grafts were with at least moderate stenosis (according to TIMI FLOW and lesion size). Use of protection devices was observed in a small percentage (13%) in an overall cohort but there has been a consistent increase in use over the years. Balloon dilatation was performed in approximately 60% of the procedures at a similar rate in the early and late division of the groups (2005-2009 and 2010-2015 respectively). The use of vasodilators was relatively high over the years (15-18%).
Regional intervention on a particular coronary artery over the years was essentially the same on LCX and RCA systems (a relatively low rate of interventions was on LAD) and that at the expense of arterial graft (LIMA) to it. A high rate of drug-coated stents has been used, especially in the recent years. Angiographic result by restored flow was achieved at a high rate in ~95% of all procedures, results were identical between the two groups. As a measure of more efficient procedure, we assessed the amount of contrast material during catheterization. Comparing average values, we observed a consistent decrease in contrast material injected during the procedure. Of course, a trend can indicate more efficient procedures and the operator’s skills.
Procedural complications were very low and this was throughout the follow-up years. Most post-procedure drug treatment was based on a combination of aspirin and Plavix. Approximately 11% of patients were treated with triple therapy including aspirin, anticoagulant, and anticoagulation therapy (coumadin). The distribution over the years has shown a decrease in the rates of a known combination of aspirin and plavix, which is mainly at the expense of an increase in the use of new antiplateletes such as prasugrel and ticagrelor.
The influence of stent type and use of protection device has been examined - it has been observed that over the years there has been a tendency to treat more severely ill patients with longer time since surgery (“older" grafts). Treatment has changed with more use of protection devices and sophisticated stents - both drug-coated and covered.
Research limitations
A major limitation may be a retrospective, single center model of the study. Notably, data on the severity of heart failure and type of stents in “prior" years are missing.
Acknowledgement: ALL the authors agree with the content of the article and with this publishing process.
Conflicts of interest: No conflict of interests is met.
Funding: The study was performed without any funding.
